

Hepatolenticular degeneration-induced hepatic dysfunction with extremely atypical clinical manifestations: a Case Report
- PMID: 40438368
- PMCID: PMC12116486
- DOI: 10.3389/fmed.2025.1599283
Hepatolenticular degeneration-induced hepatic dysfunction with extremely atypical clinical manifestations: a Case Report
Abstract
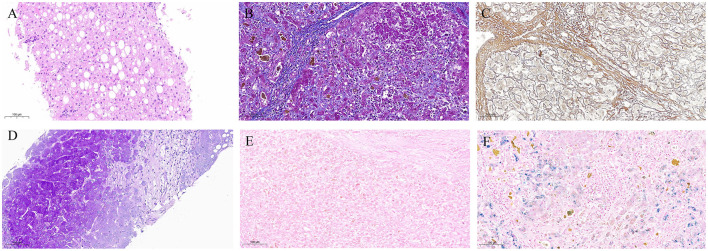
Hepatolenticular Degeneration (HLD) is a rare condition caused by a genetic copper metabolism disorder and a basal ganglia-dominated degenerative brain disease. Its characteristic clinical features include progressive extrapyramidal symptoms, psychiatric manifestations, cirrhosis, renal impairment, and the Kayser-Fleischer ring. Furthermore, its key diagnostic bases include the ceruloplasmin level, copper oxidase activity, trace copper in the human body, brain Magnetic Resonance Imaging (MRI), and genetic testing. Here, we present an HLD case with atypical clinical manifestations. A 43-year-old male HLD patient presented to our hospital with normal copper oxidase activity and serum copper levels, as well as results of ceruloplasmin testing, slit-lamp examination, and histopathological examination of the liver, which showed no typical manifestations. On the other hand, the genetic testing results showed new mutation sites. To improve our clinical understanding of HLD and reduce the probability of misdiagnosis and missed diagnosis, we discussed and clarified the clinical manifestations, pathogenesis, and diagnosis and treatment of the disease, all based on existing literature.
Keywords: atypical clinical manifestations; case report; hepatic dysfunction; hepatolenticular degeneration; whole exome sequencing.
Copyright © 2025 Tao, Zhou, Jiang, Hu, Jia and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
[The onset of psychiatric disorders and Wilson's disease].Encephale. 2007 Dec;33(6):924-32. doi: 10.1016/j.encep.2006.08.009. Epub 2007 Sep 5. Encephale. 2007. PMID: 18789784 French.
-
Genetically Confirmed Wilson Disease: A Retrospective Cohort Study From Bahrain.Cureus. 2024 Oct 18;16(10):e71805. doi: 10.7759/cureus.71805. eCollection 2024 Oct. Cureus. 2024. PMID: 39559689 Free PMC article.
-
Role for Biochemical Assays and Kayser-Fleischer Rings in Diagnosis of Wilson's Disease.Clin Gastroenterol Hepatol. 2021 Mar;19(3):590-596. doi: 10.1016/j.cgh.2020.05.044. Epub 2020 May 30. Clin Gastroenterol Hepatol. 2021. PMID: 32485301
-
Wilson Disease.1999 Oct 22 [updated 2023 Jan 12]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 1999 Oct 22 [updated 2023 Jan 12]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 20301685 Free Books & Documents. Review.
-
Four-year follow-up of a Wilson disease pedigree complicated with epilepsy and hypopituitarism: Case report with a literature review.Medicine (Baltimore). 2016 Dec;95(49):e5331. doi: 10.1097/MD.0000000000005331. Medicine (Baltimore). 2016. PMID: 27930511 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources