

Differential Characteristics and Outcomes of Urgent/Emergent Versus Elective Aortic Valve Replacement
- PMID: 40439170
- PMCID: PMC12229216
- DOI: 10.1161/JAHA.125.041148
Differential Characteristics and Outcomes of Urgent/Emergent Versus Elective Aortic Valve Replacement
Abstract
Background: Despite the slowly progressive nature of aortic stenosis, a proportion of aortic valve replacements (AVRs) still occur on an urgent/emergent basis. We sought to characterize the predictors, outcomes, and potential opportunities to prevent urgent/emergent AVRs.
Methods: We analyzed Medicare data to identify patients undergoing AVRs from 2017 to 2022. We used multivariable regression to identify factors associated with nonelective AVRs; we also examined the association of nonelective AVRs with clinical outcomes and health care costs.
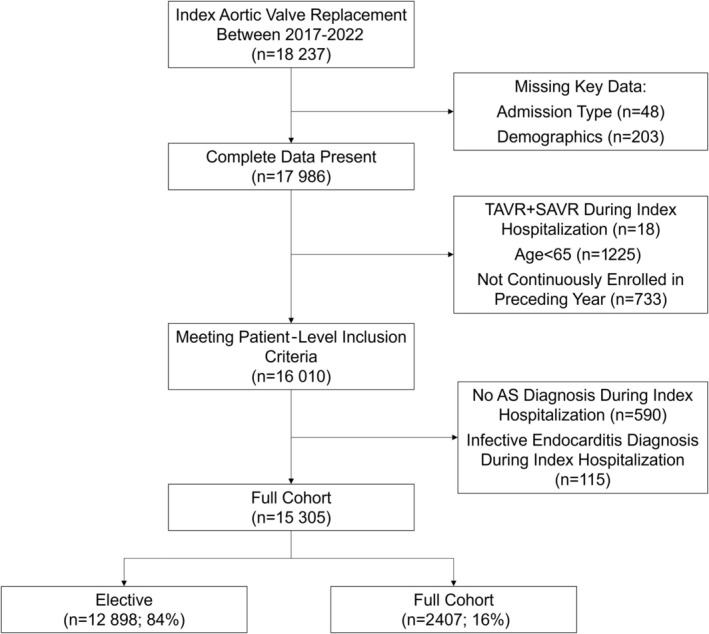
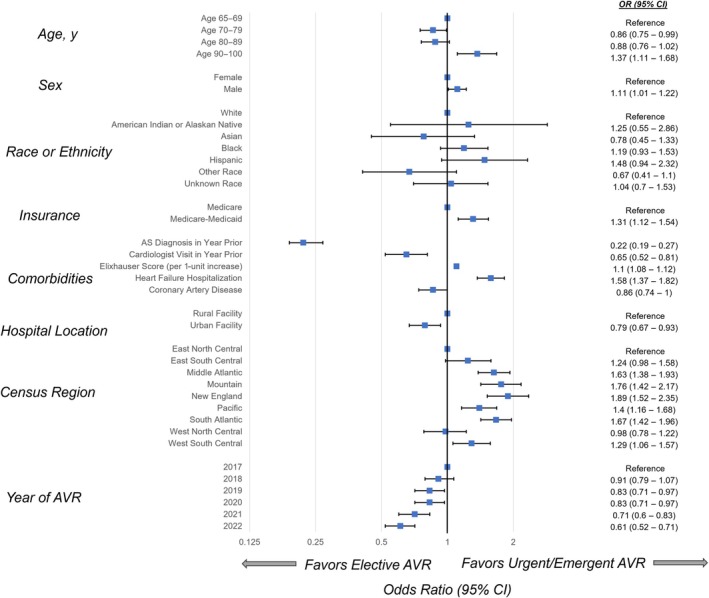
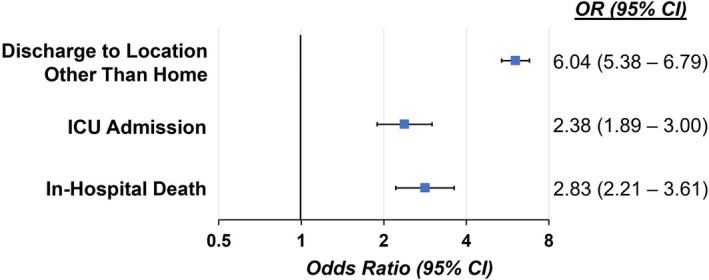
Results: In total, 15 305 patients (16% urgent/emergent) underwent AVR during the study period. Compared with patients undergoing elective AVRs, those receiving urgent/emergent AVRs were more frequently of Black race or Hispanic ethnicity, and less likely to have received a diagnosis of aortic stenosis, despite 91.7% having seen a cardiologist or primary care provider in the prior year. In multivariable-adjusted analyses, dual Medicare-Medicaid enrollment, male sex, and recent heart failure hospitalization were associated with increased risk for urgent/emergent AVR; conversely, recent aortic stenosis diagnosis and cardiologist visit were associated with lower odds of urgent/emergent AVR. In turn, urgent/emergent compared with elective AVR increased risk for in-hospital death, intensive care unit admission, and discharge to a facility versus home, in addition to longer lengths of stay and higher health care costs.
Conclusions: Urgent/emergent AVR occurs more frequently among Black, Hispanic, and dual Medicare-Medicaid-eligible patients. Nonelective AVR is also associated with worse hospital outcomes as well as greater health care costs. Importantly, variable timing in diagnosis of aortic stenosis appears to be a key determinant; thus, augmented screening efforts may improve outcomes and reduce disparities.
Keywords: Medicare; aortic valve replacement; cardiovascular outcomes; disparities.
Conflict of interest statement
Drs Kelley and Thompson and M. Platanis are Edwards Lifesciences employees. Dr Ebinger has served as a consultant and received grant funding from Edwards Lifesciences. All other authors report no relevant potential conflicts.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
