

Phase 1 studies of the indenoisoquinolines LMP776 and LMP744 in patients with solid tumors and lymphomas
- PMID: 40439882
- PMCID: PMC12122562
- DOI: 10.1007/s00280-025-04778-5
Phase 1 studies of the indenoisoquinolines LMP776 and LMP744 in patients with solid tumors and lymphomas
Abstract
Purpose: Indenoisoquinolines are a class of topoisomerase I (TOP1) inhibitors designed to overcome clinical limitations of camptothecins. Three indenoisoquinolines (LMP400, LMP776, and LMP744) demonstrated activity in murine models and a comparative canine lymphoma study. Clinical data for LMP400 were previously reported (NCT01051635). The maximum tolerated dose (MTD), safety, and clinical data from phase 1 studies of LMP776 (NCT01051635) and LMP744 (NCT03030417) are reported herein.
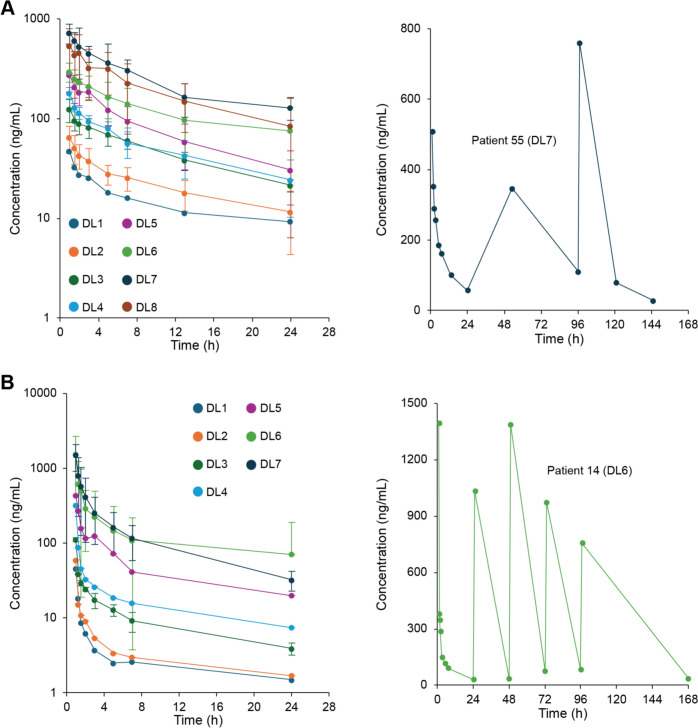
Methods: Patients ≥ 18 years of age with advanced, refractory solid tumors or lymphomas received either LMP776 (n = 34) or LMP744 (n = 35) intravenously following a Simon accelerated titration design. Both LMP776 and LMP744 were administered daily for 5 days (QDx5) in 28-day cycles. Adverse events and clinical responses were evaluated according to CTCAE and RECIST v1.1 criteria, respectively. Pharmacokinetic and pharmacodynamic changes were evaluated.
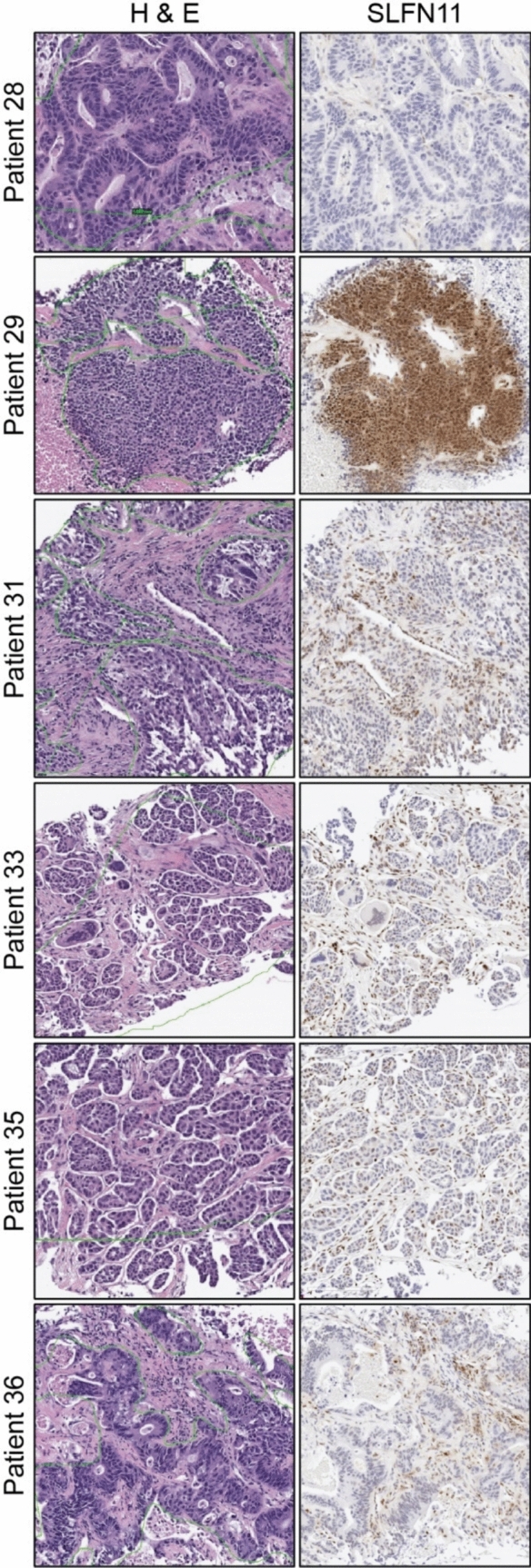
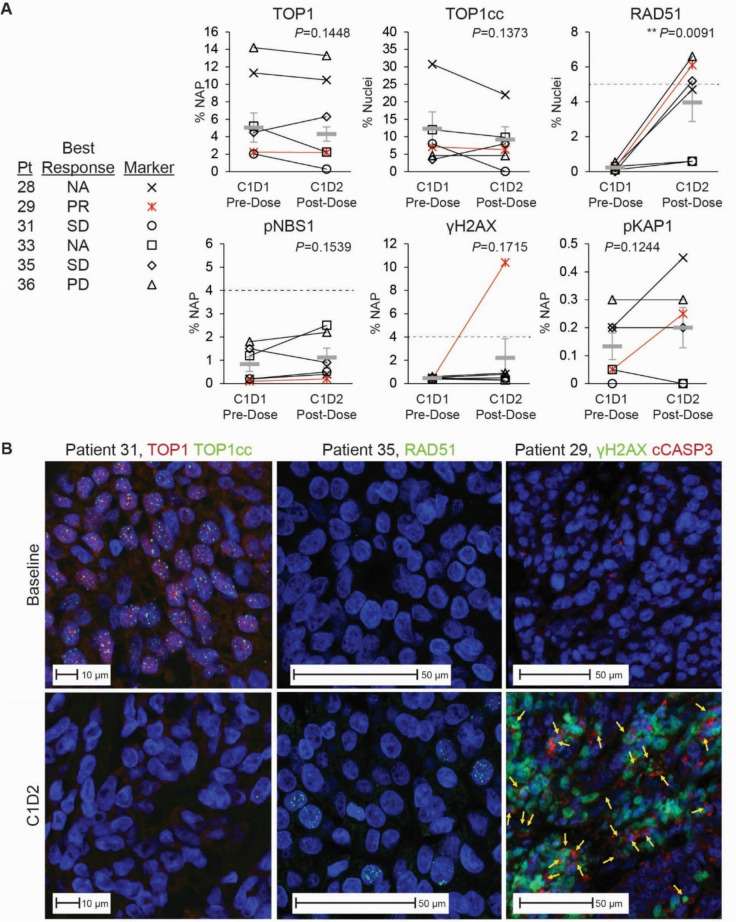
Results: The MTD of LMP776 was 12 mg/m2/day and that of LMP744 was 190 mg/m2/day. Dose-limiting toxicities (DLTs) for LMP776 included hypercalcemia, anemia, and hyponatremia; DLTs for LMP744 included hypokalemia, anemia, and weight loss. There was 1 confirmed partial response (cPR) among 35 patients receiving LMP744 (overall response rate 3%) and no objective responses in patients receiving LMP776. Tumor biopsies from the patient with cPR demonstrated high baseline expression of SLFN11 and a unique pattern of pharmacodynamic responses, including increased RAD51, phosphorylated KAP1 (pKAP1), γH2AX, and cleaved caspase-3 (cCasp3).
Conclusion: MTDs and safety profiles are reported for LMP776 and LMP744. Target engagement by an indenoisoquinoline was measured for the first time in human samples.
Keywords: Clinical trial; Indenoisoquinoline; Pharmacodynamic; Topoisomerase.
© 2025. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Declarations. Conflict of interest: Shivaani Kummar has consultant/advisory roles with Springworks Therapeutics, SeaGen, Bayer, Genome & Company, HarbourBiomed, BPGbio Therapeutics, Oxford Biotherapeutics, Mundibiopharma, BPGbio, Inc., Gilead, Mirati, Fortress Biotech, Inc., GI Innovation, Inc., Xyone Therapeutics, Genome Insight, Aadi Biosciences, MOMA Therapeutics, Daiichi Sankyo, and Pathomiq (co-founder). Other authors declare no potential conflicts of interest.
Figures

References
-
- Hsiang YH, Hertzberg R, Hecht S, Liu LF (1985) Camptothecin induces protein-linked DNA breaks via mammalian DNA topoisomerase I. J Biol Chem 260(27):14873–14878 - PubMed
-
- Wu J, Yin MB, Hapke G, Toth K, Rustum YM (2002) Induction of biphasic DNA double strand breaks and activation of multiple repair protein complexes by DNA topoisomerase I drug 7-ethyl-10-hydroxy-camptothecin. Mol Pharmacol 61(4):742–748. 10.1124/mol.61.4.742 - PubMed
-
- Caserini C, Pratesi G, Tortoreto M, Bedogne B, Carenini N, Supino R et al (1997) Apoptosis as a determinant of tumor sensitivity to topotecan in human ovarian tumors: preclinical in vitro/in vivo studies. Clin Cancer Res 3(6):955–961 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
