

Novel Hemodynamic Markers and Kidney Function in Patients with Acute Decompensated Heart Failure
- PMID: 40440457
- PMCID: PMC12136642
- DOI: 10.34067/KID.0000000703
Novel Hemodynamic Markers and Kidney Function in Patients with Acute Decompensated Heart Failure
Abstract
Key Points:
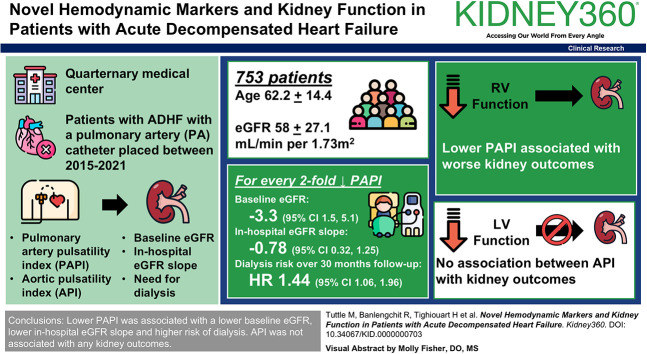
Lower pulmonary artery pulsatility index is associated with increased risk of dialysis in patients with heart failure.
No association was demonstrated between aortic pulsatility index and kidney outcomes.
Background: Patients admitted with acute decompensated heart failure are vulnerable to declines in kidney function, but the exact mechanisms are unknown. Two novel hemodynamic markers, pulmonary artery pulsatility index (PAPI) and aortic pulsatility index (API), represent composite right and left ventricular function, respectively.
Methods: Consecutive unique patient admissions for acute decompensated heart failure to a single quaternary medical center with placement of a pulmonary artery catheter between 2015 and 2021 were reviewed. Cubic spline and linear regression models were used to examine the association between these markers with baseline eGFR and in-hospital eGFR slope. Multivariate Cox proportional hazards models were used to examine the association between PAPI and API with the need for dialysis by linkage of a national database. Covariates included demographics, comorbid conditions, home medications, and baseline eGFR.
Results: The cohort included N=753 patients with mean (SD) age of 62.2 (14.4) years and eGFR of 58.0 (27.1) ml/min per 1.73 m2. For every halving of PAPI, there was a 3.3 (95% confidence interval [CI], 1.5 to 5.1) ml/min per 1.73 m2 lower baseline eGFR and a 0.78 (95% CI, 0.32 to 1.25) ml/min per 1.73 m2 per week lower in-hospital eGFR slope. Over a median follow-up time of 30.3 months, lower PAPI was associated with higher hazard of dialysis during the follow-up period (hazard ratio, 1.44 [95% CI, 1.06 to 1.96] per halving). There was no association between API with baseline eGFR, in-hospital eGFR slope, or dialysis.
Conclusions: Lower PAPI was associated with a lower baseline eGFR, lower in-hospital eGFR slope, and higher risk of dialysis. API was not associated with any kidney outcomes.
Keywords: CKD; cardiovascular disease; heart failure; hemodialysis.
Conflict of interest statement
Disclosure forms, as provided by each author, are available with the online version of the article at
Figures



References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
