

The effect of mavacamten on echocardiographic parameters, cardiac function and biomarkers in hypertrophic cardiomyopathy patients, a systematic review and meta-analysis
- PMID: 40441331
- PMCID: PMC12327524
- DOI: 10.1016/j.ihj.2025.05.011
The effect of mavacamten on echocardiographic parameters, cardiac function and biomarkers in hypertrophic cardiomyopathy patients, a systematic review and meta-analysis
Abstract
Background: Evaluate the effect of mavacamten on echocardiographic parameters and cardiac biomarkers in patients with hypertrophic cardiomyopathy (HCM).
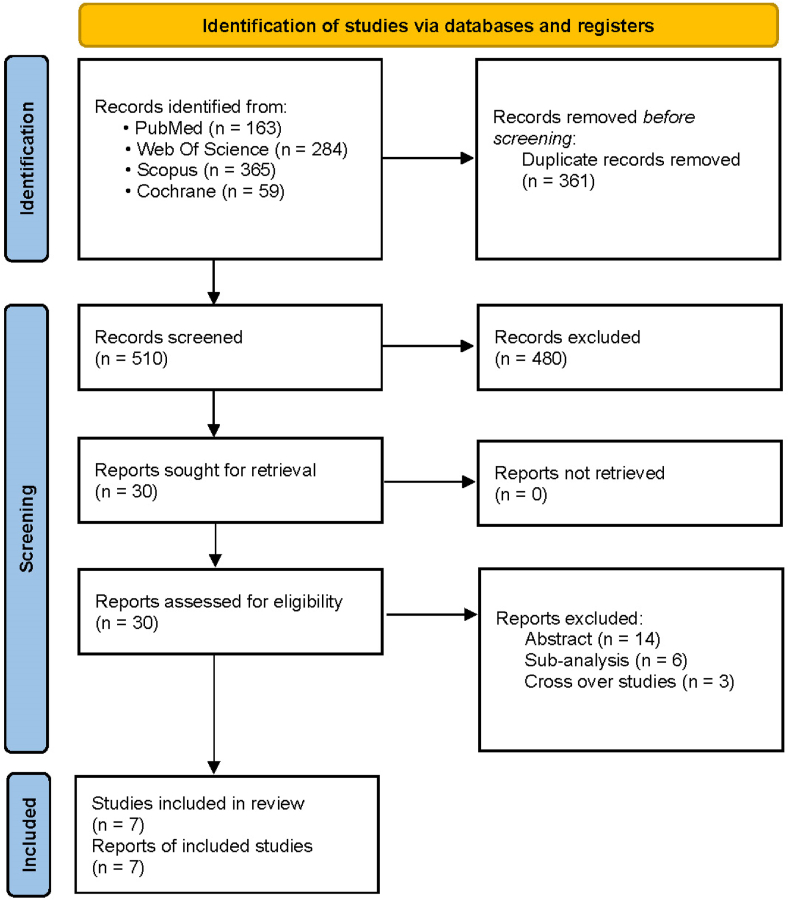
Methods: We searched PubMed, SCOPUS, Web of Science, and Cochrane Library until November 2023. Results were reported as mean difference (MD) and Risk Ratio (RR) with 95 % confidence intervals (CI).
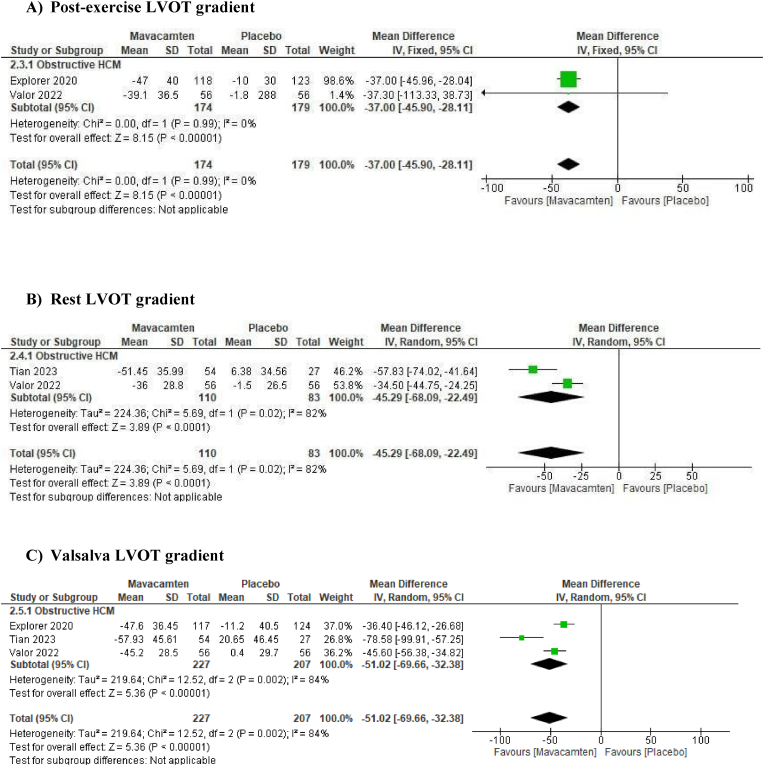
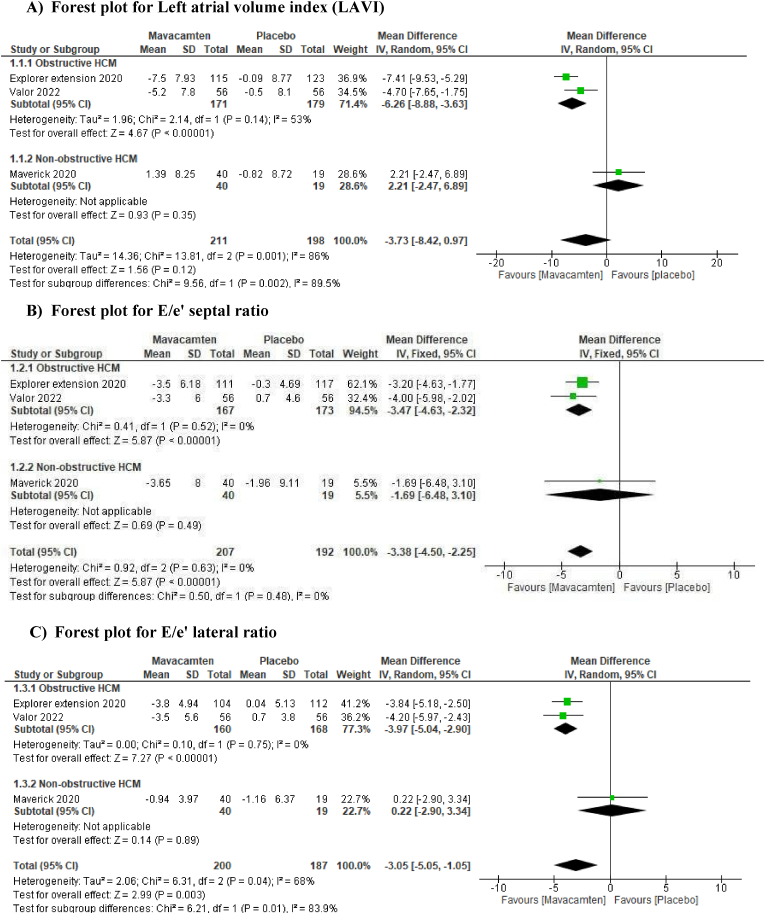
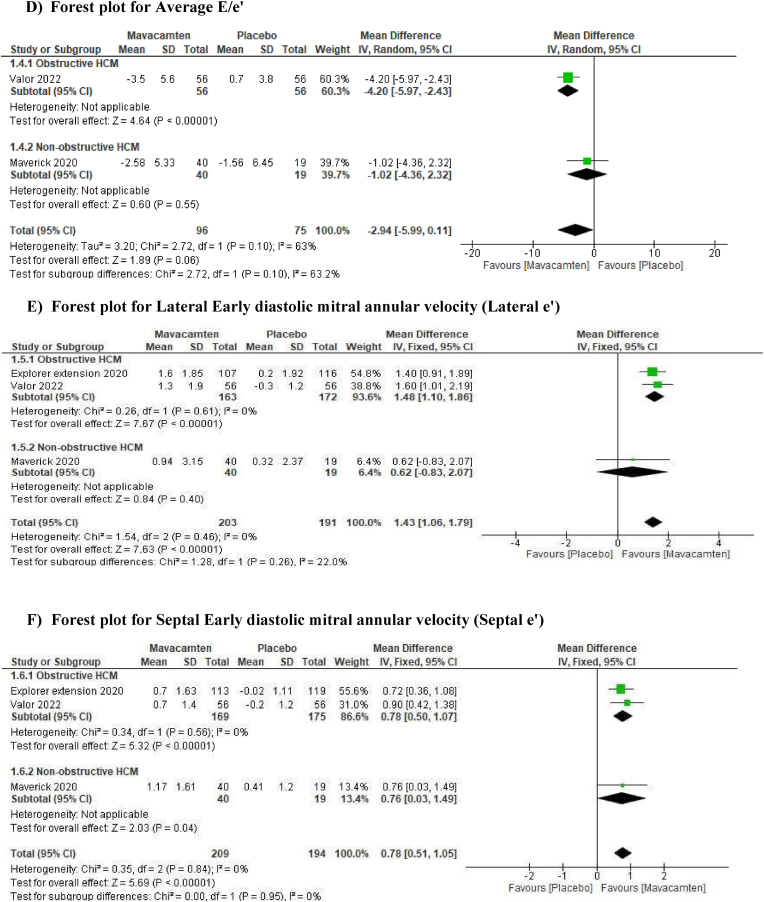
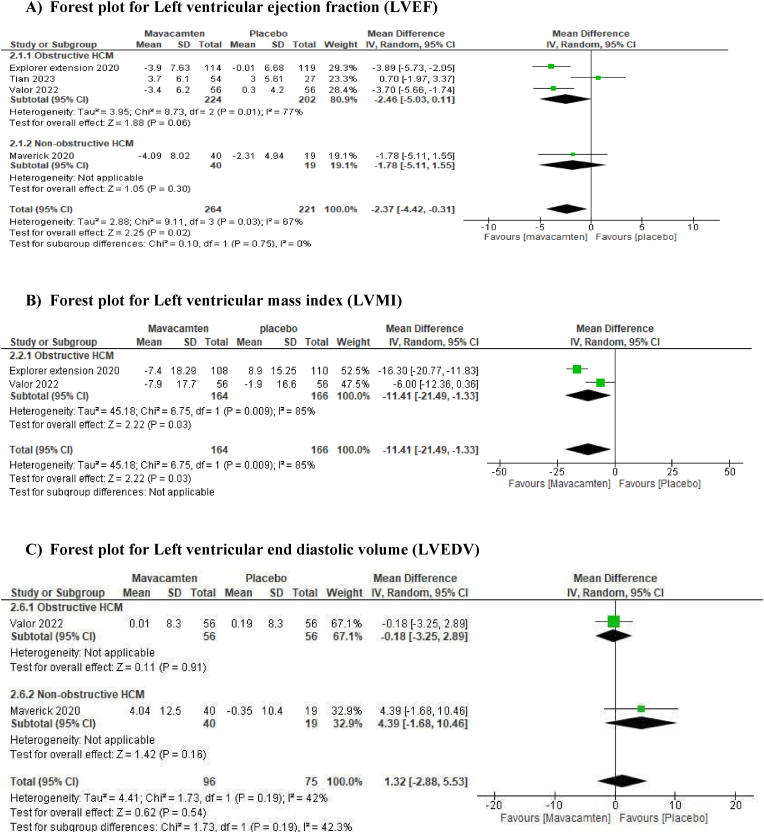
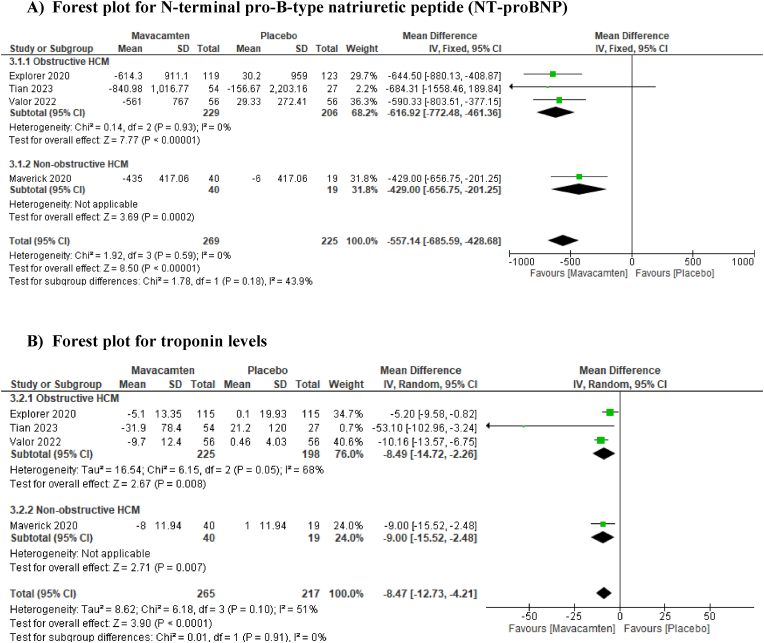
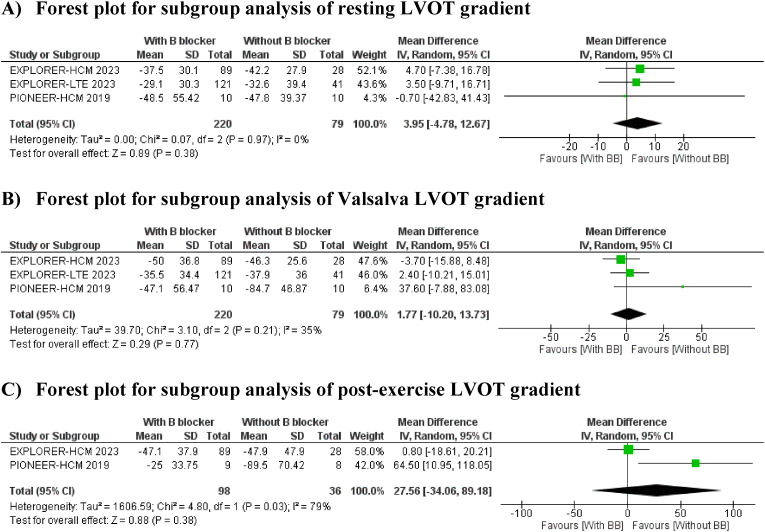
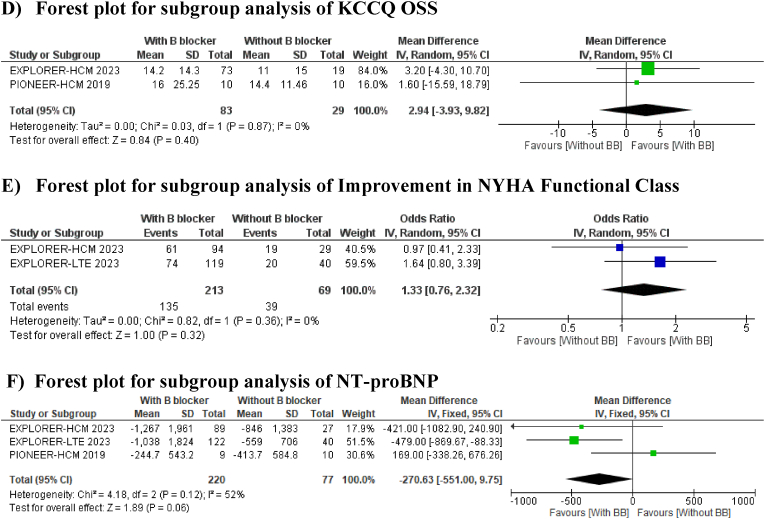
Results: Seven studies with 524 patients (456 with obstructive HCM and 59 with non-obstructive HCM) were included. Mavacamten significantly improved septal early diastolic mitral annular velocity (e') (MD 0.78, 95 % CI [0.51 to 1.05]) and left ventricular mass index (LVMI). It reduced left ventricular outflow tract (LVOT) gradient, NT-proBNP (MD -557.14, 95 % CI [-685.59 to -428.68]), and troponin levels. Improvements were also seen in left atrial volume index (MD -6.26, 95 % CI [-8.88 to -3.63]) and E/e' ratios, particularly in obstructive HCM patients.
Conclusion: Mavacamten enhances echocardiographic and cardiac biomarker outcomes in HCM patients on short-term follow-up. Limited data on non-obstructive HCM require cautious interpretation.
Keywords: Beta-blockers; Cardiac myosin inhibitor; Hypertrophic cardiomyopathy; Mavacamten.
Copyright © 2025 Cardiological Society of India. Published by Elsevier, a division of RELX India, Pvt. Ltd. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Maron B.J. Clinical course and management of hypertrophic cardiomyopathy. Longo D.L., editor. N Engl J Med. 2018;379:655–668. - PubMed
-
- Wigle E.D., Silver M.D. Myocardial fiber disarray and ventricular septal hypertrophy in asymmetrical hypertrophy of the heart. Circulation (New York, N Y) 1978;58:398–402. - PubMed
-
- Ommen S.R., Mital S., Burke M.A., et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: executive summary: a report of the American college of Cardiology/American heart association joint committee on clinical practice guidelines. Circulation (New York, N Y) 2020;142:e533–e557. - PubMed
-
- Tesic M., Seferovic J., Trifunovic D., et al. N-terminal pro-brain natriuretic peptide is related with coronary flow velocity reserve and diastolic dysfunction in patients with asymmetric hypertrophic cardiomyopathy. J Cardiol. 2017;70:323–328. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
