

Pregnant patients requiring emergency general surgery: a scoping review of diagnostic and management strategies
- PMID: 40441877
- PMCID: PMC12133296
- DOI: 10.1503/cjs.001124
Pregnant patients requiring emergency general surgery: a scoping review of diagnostic and management strategies
Abstract
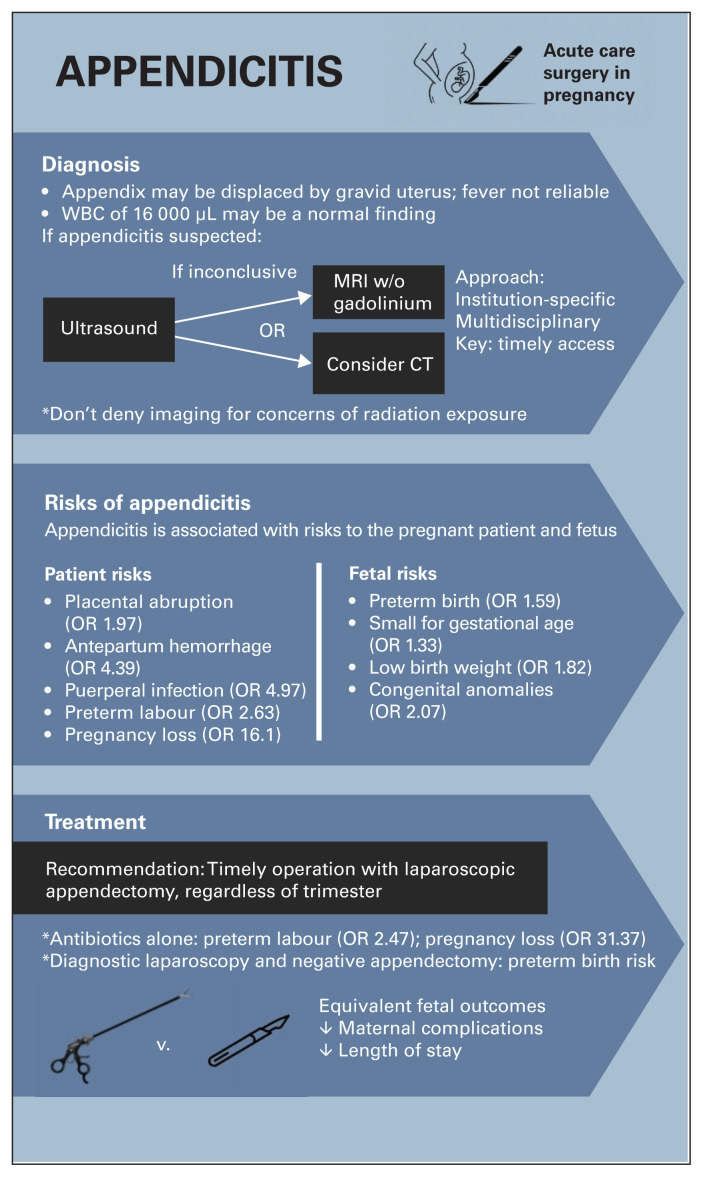
Background: About 1%-2% of pregnant patients develop conditions that require emergency general surgery (EGS). The diagnosis and management of these conditions can be challenging, as surgeons must carefully balance the needs of the pregnant patient and the developing fetus. We sought to summarize the latest literature guiding surgical management of appendicitis, benign biliary disease, bowel obstruction, and hemorrhoids in pregnant patients.
Methods: We performed a comprehensive scoping review using OVID Medline for articles published between January 2000 and June 2023 pertaining to EGS and pregnancy.
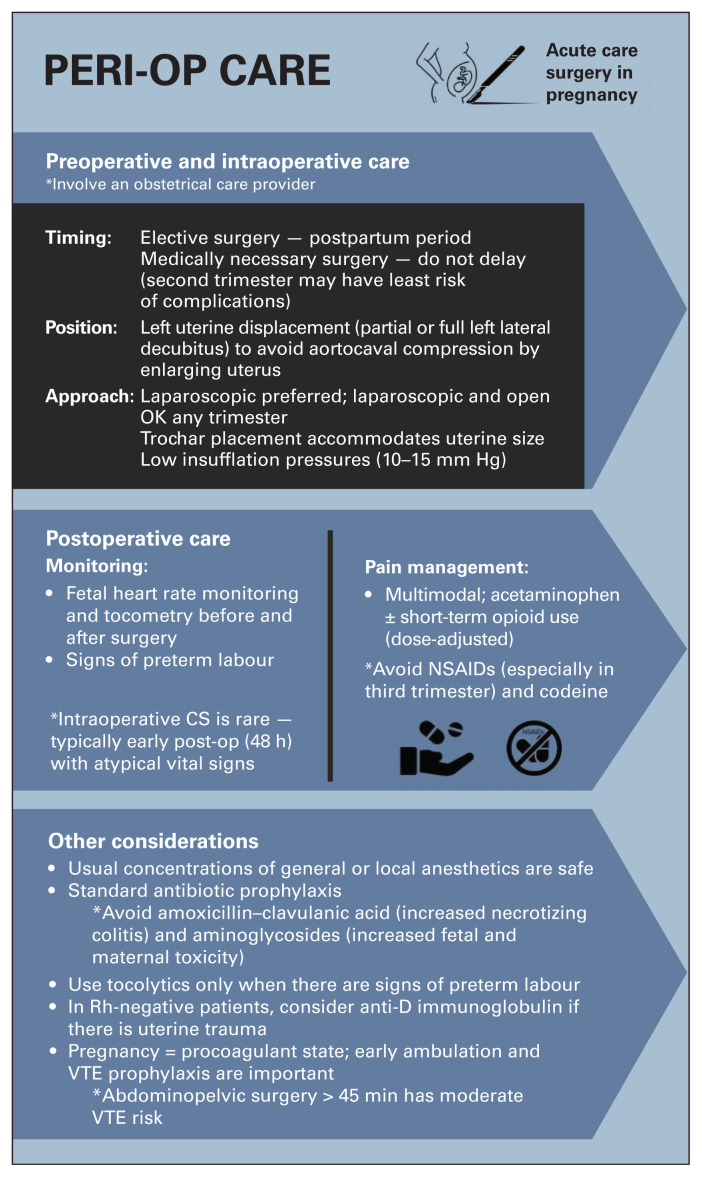
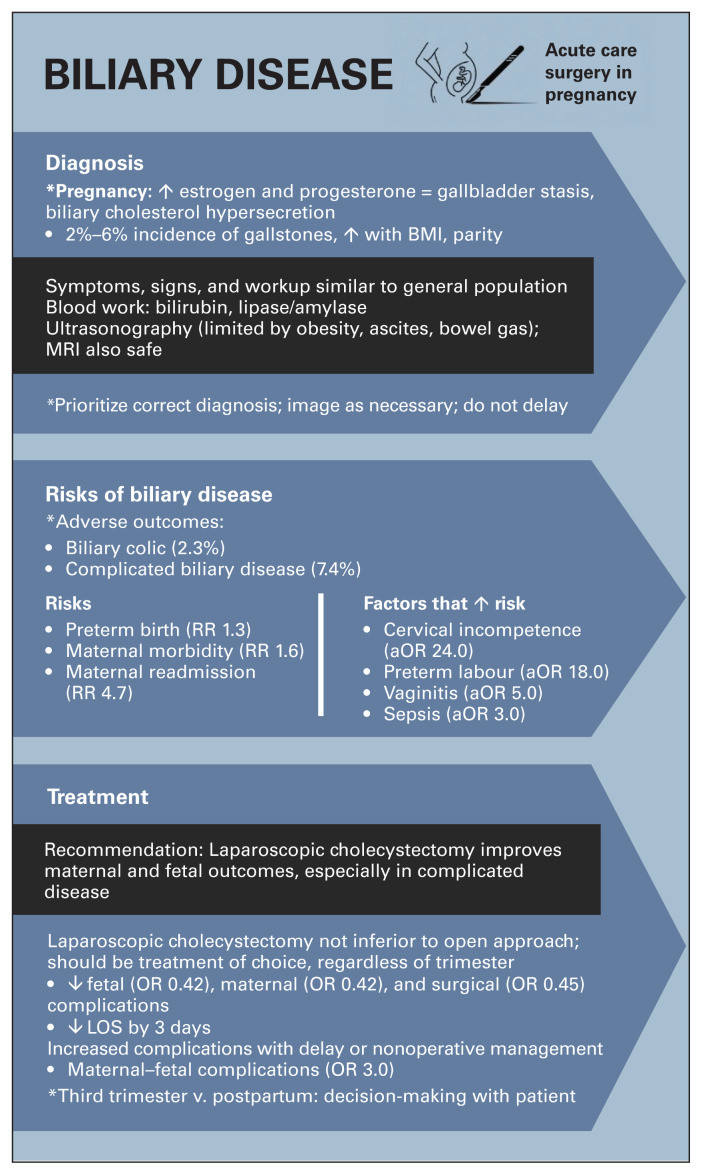
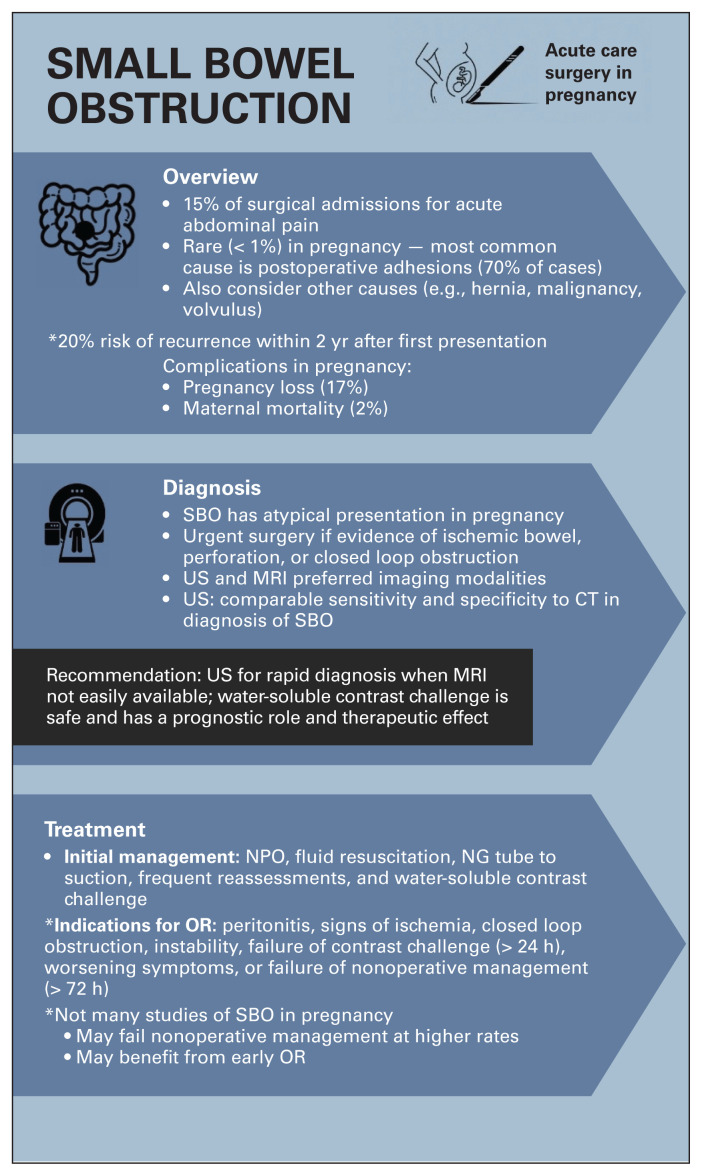
Results: Acute appendicitis, benign biliary disease, and bowel obstructions confer increased risk of adverse maternal and fetal obstetrical outcomes. In general, pregnant patients with acute appendicitis and cholecystitis should undergo appendectomy or cholecystectomy, respectively. The management of biliary colic has significant nuance depending on trimester. While an operative approach is favoured in the first 2 trimesters, the role of surgery in the third trimester is less clear. Nonoperative treatment of each of these diseases can result in significant maternal, and possibly fetal, morbidity. Operative management of bowel obstruction must be determined on a case-by-case basis. In all instances, a laparoscopic approach is preferred, if feasible.
Conclusion: A thoughtful approach is crucial for surgeons and institutions caring for pregnant patients with EGS diseases. Treatment should be similar to that in nonpregnant patients, with some important considerations and modifications. Nonoperative or delayed operative management often increases adverse obstetrical events, including death.
Contexte:: Environ 1 %–2 % des personnes enceintes devront subir une intervention urgente en chirurgie générale pour un problème de santé dont le diagnostic et la prise en charge sont parfois complexes, car il faut judicieusement prendre en compte les besoins de la personne enceinte et ceux du foetus. Nous avons voulu faire le point sur les directives récemment publiées relativement au traitement chirurgical de l’appendicite, de la maladie biliaire bénigne, de l’obstruction intestinale et des hémorroïdes chez les personnes enceintes.
Méthodes:: Nous avons procédé à une étude de portée globale à partir du réseau OVID Medline pour y trouver les articles publiés entre janvier 2000 et juin 2023 sur les interventions d’urgence en chirurgie générale et la grossesse.
Résultats:: L’appendicite, la maladie biliaire bénigne et l’obstruction intestinale aggravent le risque de complications maternelles et foetales. En général, les personnes enceintes aux prises avec une appendicite ou une cholécystite doivent subir respectivement une appendicectomie ou cholécystectomie. La prise en charge de la colique hépatique varie selon trimestre de grossesse. Une approche chirurgicale est préférable au cours des 2 premiers trimestres, mais son rôle est moins clair pour le troisième trimestre. L’approche non chirurgicale pour chacun de ces problèmes de santé peut comporter une morbidité maternelle significative et une morbidité foetale potentielle. Le recours à la chirurgie pour l’obstruction intestinale est déterminé au cas par cas. Une approche laparoscopique est toujours à privilégier si possible.
Conclusion:: Les établissements qui ont un service d’obstétrique et les équipes chirurgicales doivent impérativement adopter une approche rigoureuse face à des personnes enceintes nécessitant une intervention en chirurgie générale. Le traitement doit équivaloir à celui qui est destiné aux personnes non enceintes, moyennant certaines considérations et modifications importantes. Les modalités non chirurgicales ou un retard à les appliquer augmentent souvent le risque de complications obstétricales, y compris un risque de mortalité.
© 2025 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests:: None declared.
Figures
References
-
- Aptilon Duque G, Mohney S. Appendicitis in pregnancy. In: StatPearls 2022: Treasure Island (FL).
-
- Pastore PA, Loomis DM, Sauret J. Appendicitis in pregnancy. J Am Board Fam Med 2006;19:621–6. - PubMed
-
- Mukherjee R, Samanta S. Surgical emergencies in pregnancy in the era of modern diagnostics and treatment. Taiwan J Obstet Gynecol 2019;58:177–82. - PubMed
-
- Parangi S, Levine D, Henry A, et al. Surgical gastrointestinal disorders during pregnancy. Am J Surg 2007;193:223–32. - PubMed
-
- Challoner K, Incerpi M. Nontraumatic abdominal surgical emergencies in the pregnant patient. Emerg Med Clin North Am 2003;21:971–85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical