

Increased prevalence and risk of atherosclerotic cardiovascular disease in individuals with Type 1 diabetes and metabolic dysfunction-associated steatotic liver disease
- PMID: 40442720
- PMCID: PMC12124096
- DOI: 10.1186/s12933-025-02764-y
Increased prevalence and risk of atherosclerotic cardiovascular disease in individuals with Type 1 diabetes and metabolic dysfunction-associated steatotic liver disease
Abstract
Objective: This study aimed to investigate the correlation between metabolic dysfunction-associated steatotic liver disease (MASLD) and atherosclerotic cardiovascular disease (ASCVD) in individuals with type 1 diabetes (T1D).
Methods: Adults with T1D (n = 659) were consecutively screened for liver steatosis via abdominal ultrasound. The presence of macrovascular disease (including coronary artery disease [CAD], peripheral artery disease [PAD], or ischaemic stroke [CVA, cerebrovascular accident]) was identified via electronic medical records. The 5- and 10-year risks of fatal/nonfatal ASCVD were assessed via the Steno Type 1 Risk Engine. Insulin resistance was assessed via the estimated glucose disposal rate (eGDR).
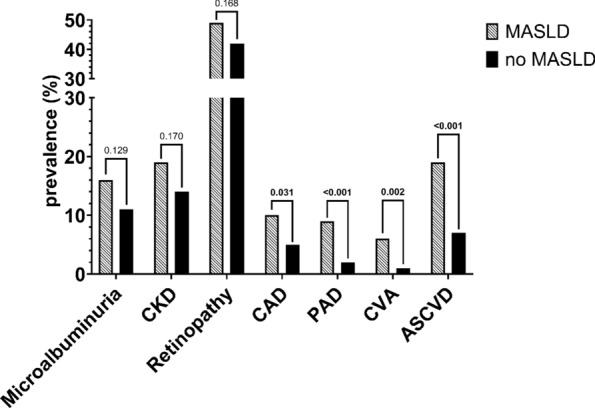
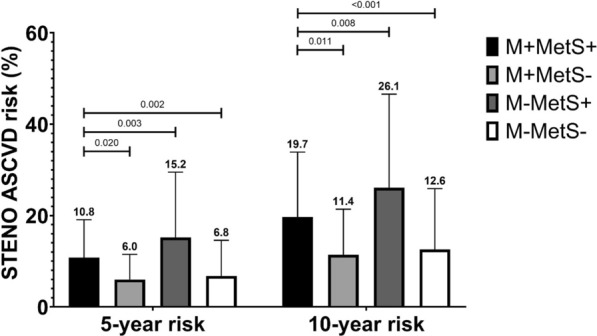
Results: The MASLD prevalence was 16.8%. The prevalence of composite ASCVD (18.9 vs. 6.8%, p < 0.001), CAD (9.9 vs. 4.7%, p = 0.031), PAD (9.0 vs. 2.2%, p < 0.001) and CVA (6.3 vs. 1.1%, p = 0.002) was greater in people with MASLD. The 5-year (7.8 [2.1-14.4] vs. 4.8 [1.6-12.0]%, p = 0.034) and 10-year (15.0 [4.1-26.8] vs. 9.4 [3.1-22.5]%, p = 0.035) risks of ASCVD were greater in those with MASLD. MASLD was associated with prevalent ASCVD (adjusted OR 4.26, 95% CI 1.79-10.11, p < 0.001), independent of age, sex, diabetes duration, smoking, statin use, LDL-cholesterol, the glomerular filtration rate, albuminuria, and metabolic syndrome.
Conclusion: MASLD is associated with both an increased prevalence of ASCVD and an increased calculated risk of fatal/nonfatal ASCVD in people with T1D.
Keywords: Atherosclerotic cardiovascular disease; Insulin resistance; MASLD; Metabolic syndrome; Type 1 diabetes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures

References
-
- Van der Schueren B, Ellis D, Faradji RN, Al-Ozairi E, Rosen J, Mathieu C. Obesity in people living with type 1 diabetes. Lancet Diabetes Endocrinol. 2021;9(11):776–85. - PubMed
-
- Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79:93. - PubMed
-
- EASL-EASD-EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J Hepatol. 2024;81(3):492–542. - PubMed
-
- Mantovani A, Csermely A, Petracca G, Beatrice G, Corey KE, Simon TG, et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(11):903–13. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
