

Comparison of thoracoscopy-guided thoracic paravertebral block and patient-controlled intravenous analgesia for postoperative analgesia after uniportal thoracoscopic pulmonary wedge resection: a prospective randomized controlled trial
- PMID: 40443516
- PMCID: PMC12119587
- DOI: 10.3389/fmed.2025.1554515
Comparison of thoracoscopy-guided thoracic paravertebral block and patient-controlled intravenous analgesia for postoperative analgesia after uniportal thoracoscopic pulmonary wedge resection: a prospective randomized controlled trial
Abstract
Introduction: Patients often experience persistent, intense pain following uniportal thoracoscopic pulmonary wedge resection (UTPWR). This pain is usually intervened with patient-controlled intravenous analgesia (PCIA) or thoracoscopic-guided thoracic paravertebral block (TG-TPB), a novel peripheral nerve block technique. Herein, we compared the analgesic effects of TG-TPB and PCIA post-UTPWR.
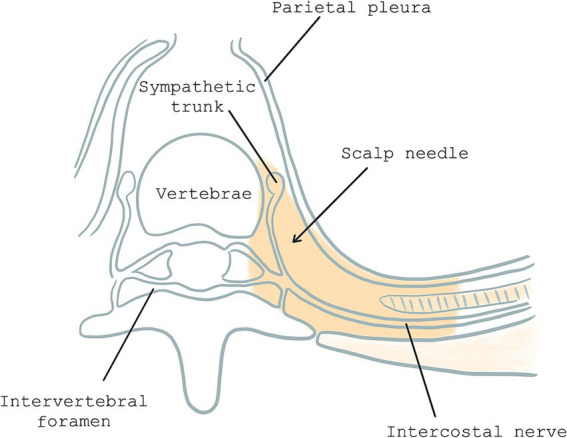
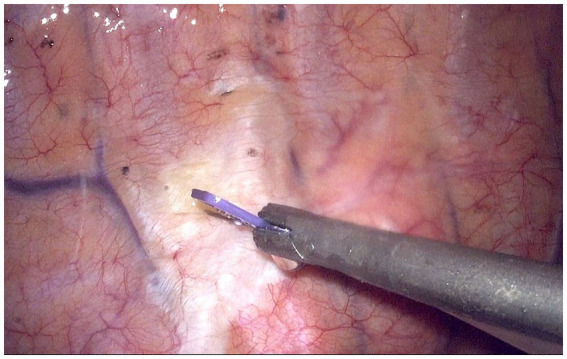
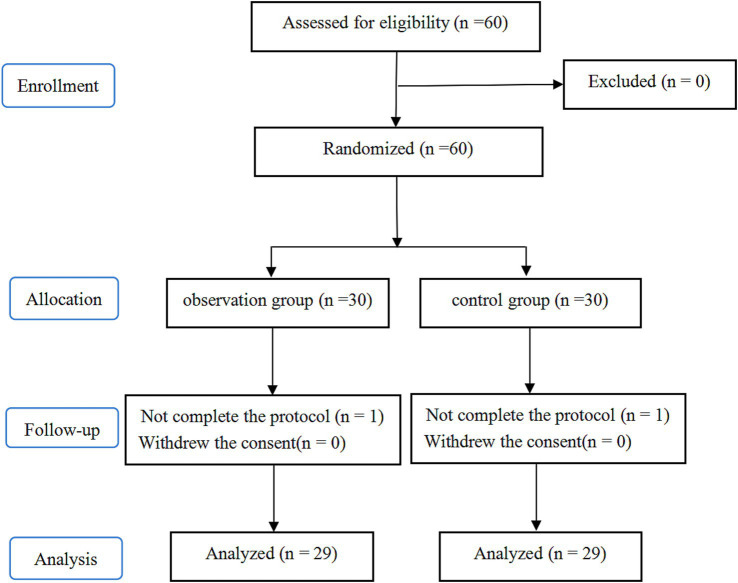
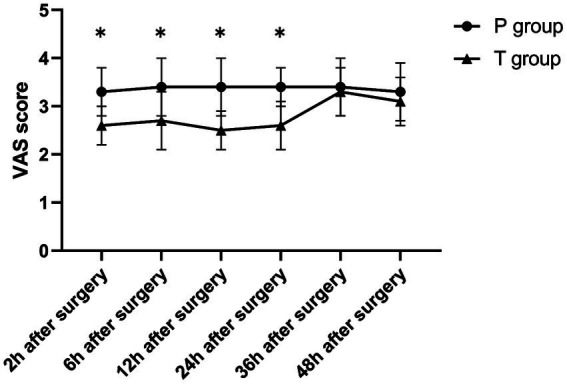
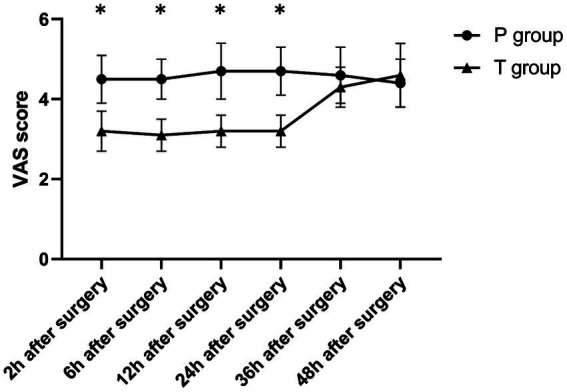
Methods: Sixty patients allocated into two groups: T and P. Group T patients were administered TG-TPB with 20 mL 0.375% ropivacaine at the fourth intercostal plane before sealing the chest, and connected to a PCIA pump containing 0.9% sodium chloride (NaCl). Group P patients received TG-TPB with 20 mL 0.9% NaCl and were connected to a PCIA pump containing sufentanil. The Visual Analogue Scale (VAS) scores were recorded at 2, 6, 12, 24, 36, and 48 h postoperatively. Data on sufentanil consumption, number of PCIA presses, number of rescue analgesia interventions, adverse reactions (ARs), and the 15-item Quality of Recovery Scale (QoR-15) scores were also recorded within 24 h postoperatively.
Results: Compared to the P group, the T group showed lower VAS scores at 2, 6, 12, and 24 h postoperatively, as well as lower sufentanil consumption levels, number of PCIA presses, number of rescue analgesia interventions, and ARs incidences within 24 h postoperatively (all p < 0.05). Furthermore, the T group showed higher QoR-15 scores within 24 h postoperatively than the P group (90.5 ± 7.3 vs. 76.6 ± 6.2; p < 0.001).
Conclusion: Compared to PCIA, TG-TPB exerted a better analgesic effect post-UTPWR, with less opioid drug use, fewer ARs, and a significantly better recovery quality within 24 h postoperatively.
Clinical trial registration: https://www.chictr.org.cn/, ChiCTR2000034726.
Keywords: patient-controlled intravenous analgesic; postoperative analgesia; pulmonary wedge resection; thoracic paravertebral block; thoracoscopic-guided; uniportal thoracoscopy.
Copyright © 2025 Du, Wei, He, Xu and Hu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comparison of postoperative analgesia by thoracoscopic-guided thoracic paravertebral block and thoracoscopic-guided intercostal nerve block in uniportal video-asssited thoracic surgery: a prospective randomized controlled trial.World J Surg Oncol. 2024 Sep 6;22(1):238. doi: 10.1186/s12957-024-03517-z. World J Surg Oncol. 2024. PMID: 39242531 Free PMC article. Clinical Trial.
-
Effect of Single-Injection Thoracic Paravertebral Block via the Intrathoracic Approach for Analgesia After Single-Port Video-Assisted Thoracoscopic Lung Wedge Resection: A Randomized Controlled Trial.Pain Ther. 2021 Jun;10(1):433-442. doi: 10.1007/s40122-020-00231-y. Epub 2021 Jan 9. Pain Ther. 2021. PMID: 33420979 Free PMC article.
-
[Application of continuous serratus plane block with patient-controlled analgesia on postoperation analgesia after thoracoscopic surgery].Zhonghua Yi Xue Za Zhi. 2018 Feb 27;98(8):570-575. doi: 10.3760/cma.j.issn.0376-2491.2018.08.003. Zhonghua Yi Xue Za Zhi. 2018. PMID: 29534383 Clinical Trial. Chinese.
-
Comparison of thoracoscopic-guided intercostal nerve block and ultrasound-guided intercostal nerve block in postoperative analgesia of uniportal video-assisted lobectomy: a pilot randomized controlled trial.Int J Surg. 2025 Feb 1;111(2):1995-2001. doi: 10.1097/JS9.0000000000002165. Int J Surg. 2025. PMID: 39705132 Clinical Trial.
-
Feasibility and effectiveness of multi-injection thoracic paravertebral block via the intrathoracic approach for analgesia after thoracoscopic-laparoscopic esophagectomy.Esophagus. 2021 Jul;18(3):513-521. doi: 10.1007/s10388-020-00807-9. Epub 2021 Jan 6. Esophagus. 2021. PMID: 33403428 Free PMC article. Clinical Trial.
References
LinkOut - more resources
Full Text Sources
Miscellaneous