

The brain shock index: repurposing the Lindegaard ratio for detecting cerebral hypoperfusion in children with cerebral malaria
- PMID: 40445535
- PMCID: PMC12125453
- DOI: 10.1186/s13089-025-00430-8
The brain shock index: repurposing the Lindegaard ratio for detecting cerebral hypoperfusion in children with cerebral malaria
Abstract
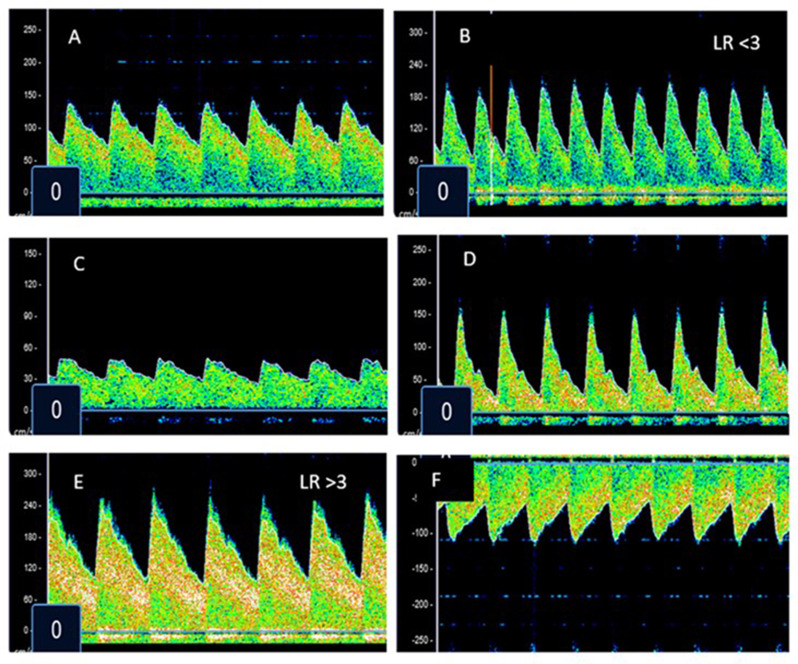
Background: Transcranial doppler ultrasound (TCD) allows for the assessment of the cerebrovascular hemodynamics in critically ill children. Given the increasing availability of machines equipped with TCD capabilities globally, it may be a useful approach to detect cerebral hypoperfusion and guide neurologic resuscitation for pediatric patients in resource limited settings where other neuromonitoring techniques are unavailable. However, the current need to evaluate waveform characteristics and to age correct values to determine if a study is abnormal decreases the feasibility of using point of care TCD in this way. The brain shock index (BSI), a repurposing of the Lindegaard Ratio, overcomes these limitations.
Methods: We performed a prospective study of children with cerebral malaria (CM). On admission and daily thereafter, TCD was used to evaluate the middle cerebral (MCA) and extra-cranial carotid arteries (Ex-ICA), and the BSI was calculated bilaterally (MCA mean flow velocity ((Vm))/Ex-ICA Vm). Neurologic outcome at discharge was assessed.
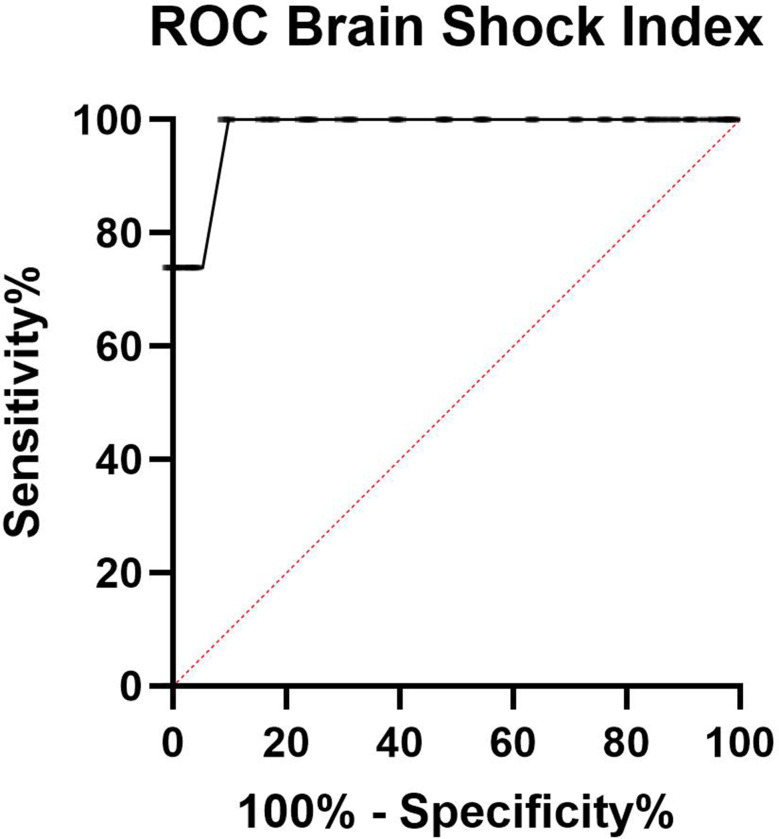
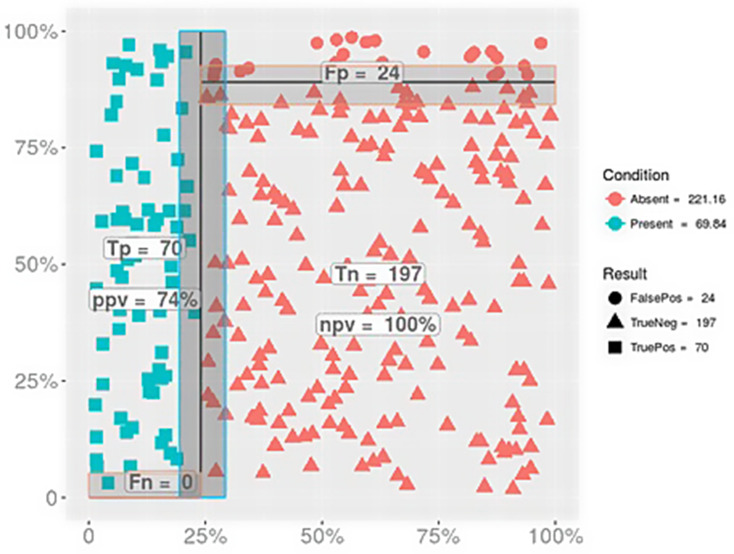
Results: A cohort of 291 children with CM were evaluated. BSI calculation was successful in all of them. The mean time to perform TCD and calculate the BSI was 4 ± 2 min. Overall, 222 participants (76%) had a good outcome and 69 (24%) a poor outcome. The BSI had an AUC of 0.98 (95% CI 0.97-0.99, p < 0.0001) to predict death or moderate to severe disability. The highest sensitivity and specificity of the BSI to predict adverse outcomes occurred at a cut off value ≤ 1.1. The adjusted odds ratio of poor outcome was 3.2 (95% CI 1.6-6.1, p = 0.001) if any BSI measurement during hospitalization fell below this threshold. No intracranial pressure monitoring was available to determine the relationship between the BSIs and an invasively measured cerebral perfusion pressure.
Conclusion: The BSI is a rapid, feasible point of care ultrasound measurement of cerebral hypoperfusion, with values ≤ 1.1 strongly correlating with poor neurologic outcomes in children with CM. Future studies should be performed to assess the utility of BSI to detect the presence and measure the severity of reduced cerebral perfusion pressure in other populations of critically ill children.
Keywords: BSI; Brain shock; Brain shock index; POCUS; TCD; Transcranial doppler ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: was obtained in each country (DRC CES ID 279/CNES/BN/PMMF/2021, Zambia ERES ID 00005948, Malawi COMREC P.04/24–0650). Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Noninvasive screening for intracranial hypertension in children with acute, severe traumatic brain injury.J Neurosurg Pediatr. 2015 Oct;16(4):420-5. doi: 10.3171/2015.3.PEDS14521. Epub 2015 Jul 3. J Neurosurg Pediatr. 2015. PMID: 26140576
-
[The usefulness of transcranial Doppler ultrasonography in the early phase of head injury].Neurocirugia (Astur). 2002 Jun;13(3):196-208. doi: 10.1016/s1130-1473(02)70617-9. Neurocirugia (Astur). 2002. PMID: 12148164 Clinical Trial. Spanish.
-
Assessment of intracranial venous blood flow after subarachnoid hemorrhage: a new approach to diagnose vasospasm with transcranial color-coded duplex sonography.J Neurosurg. 2018 Nov 1;129(5):1136-1142. doi: 10.3171/2017.5.JNS17232. Epub 2017 Dec 15. J Neurosurg. 2018. PMID: 29243981
-
Transcranial Doppler ultrasonography in neurological surgery and neurocritical care.Neurosurg Focus. 2019 Dec 1;47(6):E2. doi: 10.3171/2019.9.FOCUS19611. Neurosurg Focus. 2019. PMID: 31786564 Review.
References
-
- Aaslid R, Markwalder TM, Nornes H (1982) Noninvasive transcranial doppler ultrasound recording of flow velocity in basal cerebral arteries. J Neurosurg 57:769–774 - PubMed
-
- Aaslid R, Lindegaard KF, Sorteberg W, Nornes H (1989) Cerebral autoregulation dynamics in humans. Stroke 20:45–52 - PubMed
-
- O’Brien NF, Buttram SDW, Maa T et al (2019) Cerebrovascular physiology during pediatric extracorporeal membrane oxygenation: A multicenter study using transcranial doppler ultrasonography. Pediatr Crit Care Med 20:178–186 - PubMed
-
- O’Brien NF, Maa T, Reuter-Rice K (2015) Noninvasive screening for intracranial hypertension in children with acute, severe traumatic brain injury. J Neurosurg Pediatr 16:420–425 - PubMed
-
- LaRovere KL, O’Brien NF, Tasker RC (2016) Current opinion and use of transcranial doppler ultrasonography in traumatic brain injury in the pediatric intensive care unit. J Neurotrauma 33:2105–2114 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous