

Understanding the hemodynamic changes in fetuses with coarctation of the aorta using a lumped model of fetal circulation
- PMID: 40446209
- PMCID: PMC12124859
- DOI: 10.1371/journal.pcbi.1013096
Understanding the hemodynamic changes in fetuses with coarctation of the aorta using a lumped model of fetal circulation
Abstract
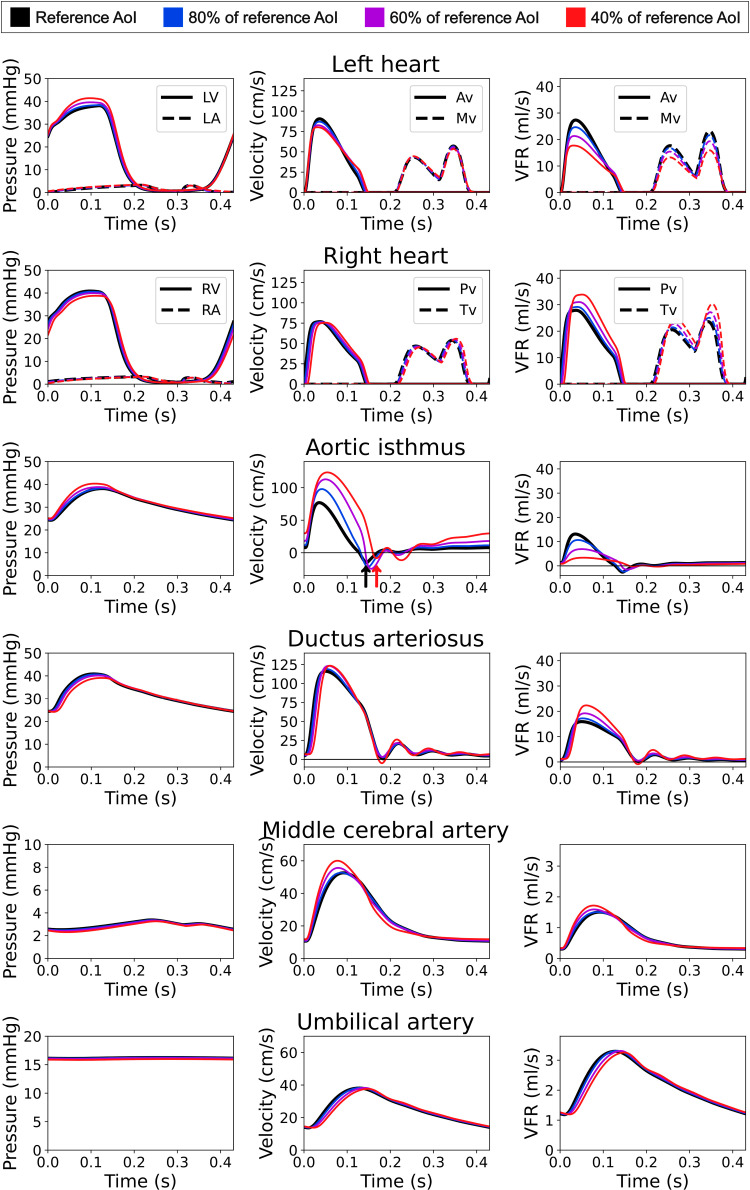
Coarctation of the aorta (CoA) is a common congenital heart defect characterized by aortic narrowing. Prenatally, it has mild hemodynamic effects as right ventricular disproportion and ductus arteriosus (DA) dilation occur as adaptive mechanisms, but their impact on CoA hemodynamics remains poorly understood. To investigate this, we built a closed 0D computational model of fetal circulation and simulated different CoA cardiovascular remodeling patterns, including aortic isthmus (AoI) narrowing, ventricular disproportion, and DA dilation. Our results showed mild AoI narrowing (80% of reference diameter) required up to 1.7 right/left ventricular end-diastolic volume ratio and 115% DA dilation to maintain physiological pressures, wall shear stresses, and organ perfusion. In contrast, severe narrowing (20% of reference AoI diameter) required up to 5 right/left ventricular end-diastolic volume ratio and 125% DA dilation, highlighting the necessity of co-occurrence of prenatal ventricular disproportion and DA dilation to compensate for AoI narrowing. These physiological regions were validated with ultrasonographic measurements from 7 controls and 9 CoA patients. We compared blood pressures, velocities, and volumetric flow rates across different fetoplacental anatomical sites. AoI velocity showed a delayed retrograde flow peak and increased antegrade diastolic velocity with greater AoI narrowing, which may aid in diagnosing CoA. Minimal differences were observed in other velocities and pressures. Volumetric flow rates across varying degrees of AoI narrowing decreased in the AoI and mitral and aortic valves, remained stable in the middle cerebral and umbilical arteries, and increased in the DA and tricuspid and pulmonary valves. Therefore, we corroborated that in fetal CoA a redistribution of blood flow occurs to ensure perfusion of the brain and placenta, without a significant alteration in fetal hemodynamics (blood pressure and velocities) except for increased diastolic velocities in the AoI.
Copyright: © 2025 Villanueva-Baxarias et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
The Diastolic and Systolic Velocity-Time Integral Ratio of the Aortic Isthmus Is a Sensitive Indicator of Aortic Coarctation in Fetuses.J Am Soc Echocardiogr. 2019 Nov;32(11):1470-1476. doi: 10.1016/j.echo.2019.06.011. Epub 2019 Aug 20. J Am Soc Echocardiogr. 2019. PMID: 31443942
-
Is retrograde blood flow of aortic isthmus useful for the prenatal screening of coarctation of the aorta by fetal color Doppler echocardiography? A preliminary study.J Med Ultrason (2001). 2018 Jul;45(3):431-435. doi: 10.1007/s10396-017-0844-z. Epub 2017 Nov 23. J Med Ultrason (2001). 2018. PMID: 29170884
-
Fetal sheep central haemodynamics and cardiac function during occlusion of the ascending aorta.Exp Physiol. 2018 Jan 1;103(1):58-67. doi: 10.1113/EP086500. Epub 2017 Dec 3. Exp Physiol. 2018. PMID: 29094424
-
Diagnostic accuracy of prenatal ultrasound in coarctation of aorta: systematic review and individual participant data meta-analysis.Ultrasound Obstet Gynecol. 2024 Apr;63(4):446-456. doi: 10.1002/uog.27576. Epub 2024 Mar 9. Ultrasound Obstet Gynecol. 2024. PMID: 38197327
-
Aortic Isthmus Doppler Velocimetry in Fetuses with Intrauterine Growth Restriction: A Literature Review.Rev Bras Ginecol Obstet. 2020 May;42(5):289-296. doi: 10.1055/s-0040-1710301. Epub 2020 May 29. Rev Bras Ginecol Obstet. 2020. PMID: 32483809 Free PMC article. Review.
References
-
- Keshavarz-Motamed Z, Edelman ER, Motamed PK, Garcia J, Dahdah N, Kadem L. The role of aortic compliance in determination of coarctation severity: Lumped parameter modeling, in vitro study and clinical evaluation. J Biomech. 2015;48(16):4229–37. doi: 10.1016/j.jbiomech.2015.10.017 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
