

Clinicians' lived experience of concealing bad news: a qualitative study in Malaysia and the UK
- PMID: 40447427
- PMCID: PMC12128409
- DOI: 10.1136/bmjopen-2024-094589
Clinicians' lived experience of concealing bad news: a qualitative study in Malaysia and the UK
Abstract
Objective: Clinicians acknowledge that receiving bad news is challenging and life-altering, while recognising that candid communication is needed for effective patient care. In some cultures, patients' relatives commonly ask doctors to hide bad news, with the intention of reducing psychological distress. Although well-intentioned, concealing information has harmful consequences for the patient, their caregivers and the healthcare team. Our study focuses on clinicians' lived experience of this phenomenon. Previous research has provided some exploration of how practitioners navigate this dilemma. Our study aims to deepen understanding, with two goals: improving cultural competence when facing this dilemma and equipping clinicians to navigate this professional challenge.
Design: As this study explored lived experience, we drew on the methodology of phenomenology. To allow deep insight into how clinicians navigate this dilemma, participants took part in focus groups and semistructured interviews. Interviews were audiorecorded, transcribed and analysed using thematic content analysis. The study was strongly influenced by the work of Braun and Clarke, who emphasise the strength in subjectivity in qualitative research. Reporting was guided by the COnsolidated criteria for REporting Qualitative research.
Settings: Recognising that this practice varies significantly across cultures, we recruited clinicians who had experienced a cultural challenge: medical students receiving a UK curriculum in Malaysia and the UK and international medical graduates working in the UK.
Participants: 26 medical students and 16 international medical graduates participated.
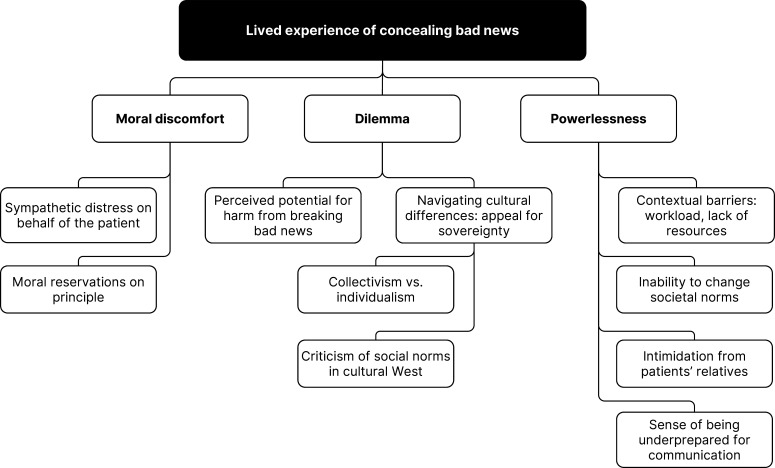
Results: For our participants, concealing diagnoses created multiple sources of personal distress. Three major themes emerged: moral discomfort, dilemma and powerlessness. Sympathetic distress at the impact on the patient was stark. However, conflicting personal and professional values created uncertainty. Some of our participants shared the relatives' concern that diagnostic disclosure could potentially harm the patient. Even when our participants wanted to disclose diagnoses, they felt underequipped for communication challenges and faced coercion to conceal information, generating a professional dilemma and a sense of powerlessness.
Conclusion: The crucial next step is for medical education to acknowledge that requests to conceal diagnoses happen. We need to provide a communication strategy for tackling this phenomenon, which upholds the patient's right to knowledge while maintaining collaboration and trust with the patient's family. Furthermore, this dilemma highlights shortcomings in our current approach to teaching medical ethics. Our findings offer globalised healthcare education an opportunity for self-awareness. Learning from and respecting global variation shines a light on our biases, allowing progress towards curriculum decolonisation.
Keywords: MEDICAL EDUCATION & TRAINING; MEDICAL ETHICS; PALLIATIVE CARE.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Doctors' Perceptions and Practices of Breaking Bad News: A Qualitative Study From Greece.Health Commun. 2017 Jun;32(6):657-666. doi: 10.1080/10410236.2016.1167991. Epub 2016 Jul 1. Health Commun. 2017. PMID: 27367603
-
Disclosure of true medical information: the case of Bangladesh.BMC Med Ethics. 2024 Oct 17;25(1):112. doi: 10.1186/s12910-024-01115-y. BMC Med Ethics. 2024. PMID: 39415215 Free PMC article.
-
Breaking bad news: tackling cultural dilemmas.BMJ Support Palliat Care. 2021 Jun;11(2):128-132. doi: 10.1136/bmjspcare-2020-002700. Epub 2021 Mar 24. BMJ Support Palliat Care. 2021. PMID: 33762267
-
[Are schizophrenic patients being told their diagnosis today in France?].Encephale. 2017 Apr;43(2):160-169. doi: 10.1016/j.encep.2016.01.011. Epub 2016 Jun 29. Encephale. 2017. PMID: 27372353 Review. French.
-
Thinking ahead about medical treatments in advanced illness: a qualitative study of barriers and enablers in end-of-life care planning with patients and families from ethnically diverse backgrounds.Health Soc Care Deliv Res. 2023 Jun;11(7):1-135. doi: 10.3310/JVFW4781. Health Soc Care Deliv Res. 2023. PMID: 37464868
Cited by
-
Transnational medical education programmes and preparation for different country medical practice: A systematic review.Med Educ. 2025 Sep;59(9):924-937. doi: 10.1111/medu.15660. Epub 2025 Mar 22. Med Educ. 2025. PMID: 40119725 Free PMC article. Review.
References
-
- Tsoussis S, Papadogiorgaki M, Markodimitraki E, et al. Disclosure of cancer diagnosis: the Greek experience. J BUON. 2013;18:516–26. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials