

Effects of dynamic stabilization and fusion on postoperative paraspinal muscle degeneration and lumbar function recovery
- PMID: 40448178
- PMCID: PMC12125767
- DOI: 10.1186/s13018-025-05837-6
Effects of dynamic stabilization and fusion on postoperative paraspinal muscle degeneration and lumbar function recovery
Abstract
Objective: To investigate the relationship between segmental motion and paraspinal muscle degeneration at the surgical level in patients with single-level lumbar degenerative disease (LDD) who have undergone either fusion or dynamic stabilization surgery.
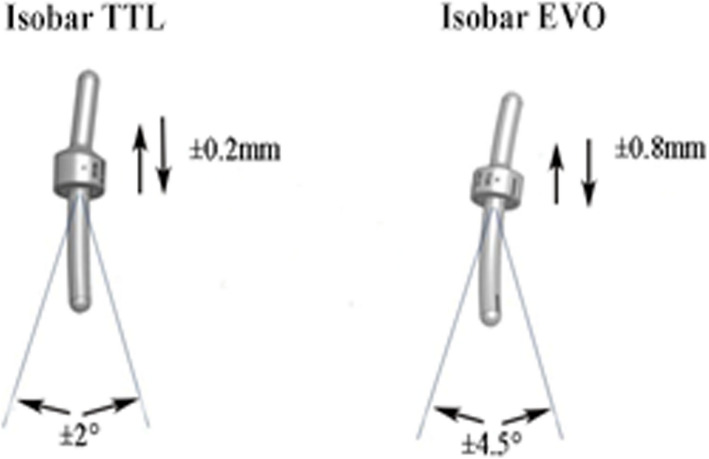
Methods: Patients treated with posterolateral intertransverse fusion (PITF group), Isobar TTL dynamic internal fixation (TTL group), or Isobar EVO dynamic internal fixation (EVO group) for single-level lumbar degenerative disease (LDD) between March 2012 and September 2020 were included in the study. Cases were selected with complete records and follow-up times ranging from 2 to 5 years, taking into account the effects of postoperative muscle edema and age-related muscle degeneration. The study compared operative time, intraoperative blood loss, preoperative and postoperative Oswestry Disability Index (ODI) scores, Lumbar Stiffness Disability Index (LSDI) scores, range of motion (ROM) at the surgical segment, cross-sectional area (CSA) of the paraspinal muscles, and functional cross-sectional area (FCSA) of the paraspinal muscles before and after surgery across all groups.
Results: A total of 73 patients were included in this study: 23 in the PITF group, 26 in the TTL group, and 24 in the EVO group. There were no statistically significant differences among the three groups in terms of age, gender, follow-up duration, body mass index (BMI), preoperative lumbar VAS score, preoperative ODI score, and preoperative LSDI score (P > 0.05). Postoperative ODI scores were significantly higher in the PITF group compared to the TTL and EVO groups, with ODI scores demonstrating a moderate negative correlation with postoperative range of motion (ROM) of the surgical segment (Pearson's r = -0.333, P < 0.004). A strong negative monotonic relationship was observed between ROM of the surgical segment and the rate of change in functional cross-sectional area (FCSA) of the paraspinal muscles across all groups, as evidenced by Spearman's correlation coefficients (PITF: r = -0.766, P < 0.001; TTL: r = -0.818, P < 0.001; EVO: r = -0.865, P < 0.001) (Fig. 7). Multiple linear regression models confirmed that age, BMI, and gender had no significant effect on the rate of FCSA change. For the PITF, TTL, and EVO groups, the regression coefficients for ROM's association with FCSA change were β = -0.653 (P < 0.005), β = -0.956 (P < 0.001), and β = -0.908 (P < 0.001), respectively. Similarly, postoperative LSDI scores were significantly elevated in the PITF group compared to the TTL and EVO groups, with LSDI scores exhibiting a strong negative correlation with postoperative ROM (r = -0.802, P < 0.001).
Conclusion: Compared to traditional decompression combined with rigid fusion surgery, decompression coupled with dynamic stabilization techniques can more effectively alleviate postoperative lumbar stiffness and functional impairment in patients. Moderately enhancing the range of motion at the surgical level facilitates the remodeling of paraspinal muscle tissue following surgery.
Keywords: Isobar; Lumbar degenerative disease; Paraspinal muscles fat infiltration; Posterior pedicle screw fixation; Posterolateral intertransverse lumbar fusion.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures







References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
