

Cross-organ hierarchy of HLA molecular mismatches in donor-specific antibody development in solid organ transplantations
- PMID: 40449481
- PMCID: PMC12208338
- DOI: 10.1016/j.xcrm.2025.102153
Cross-organ hierarchy of HLA molecular mismatches in donor-specific antibody development in solid organ transplantations
Abstract
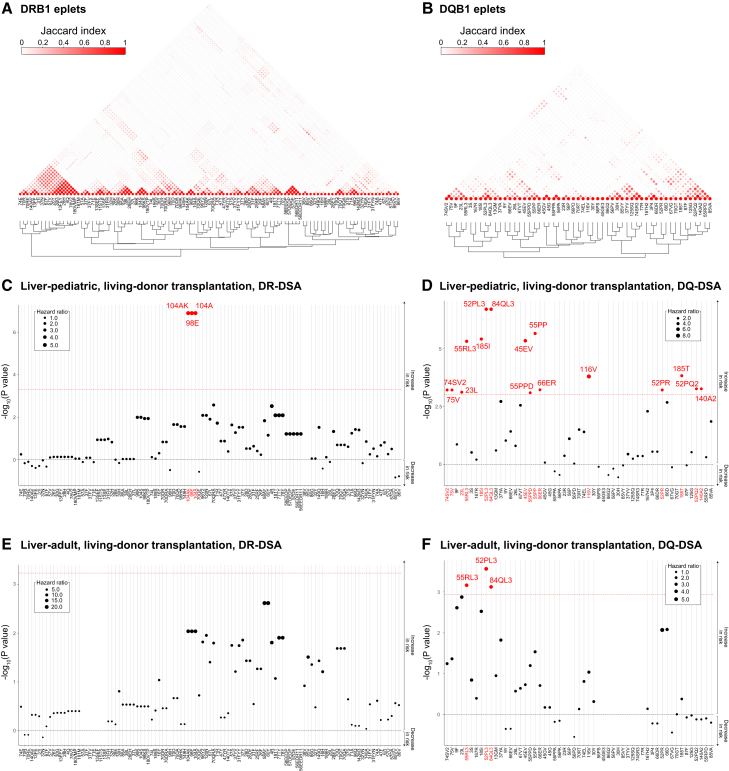
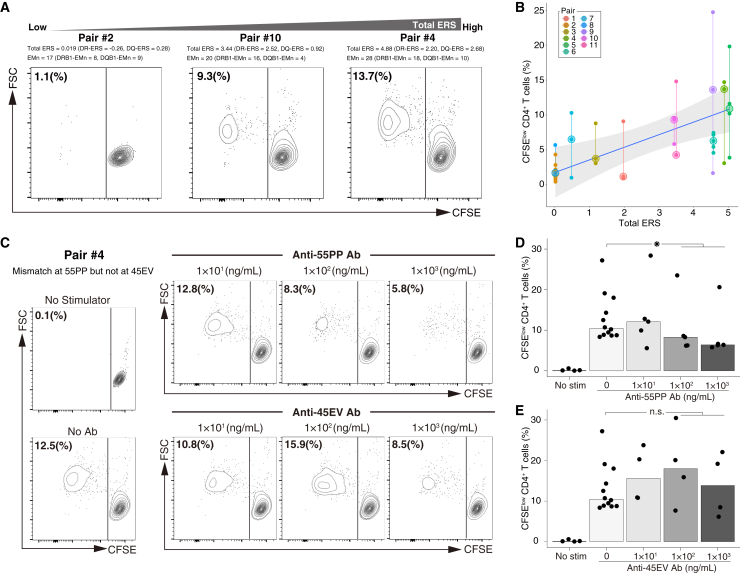
Donor-specific antibodies (DSAs) against human leukocyte antigen (HLA) play a crucial role in antibody-mediated rejection, a major barrier to successful organ transplantation. Donor-recipient HLA molecular incompatibility critically influences DSA susceptibility, commonly assessed by analyzing mismatches in the HLA eplet repertoire. This study, including six distinct liver, lung, and kidney transplant cohorts from two centers (978 donor-recipient pairs), explores associations between individual eplet mismatches and DSA development. Certain mismatched eplets are strongly linked to DSA development, while others show weaker associations, a trend consistent across different organ types. Machine learning leverages these hierarchical associations to develop an eplet risk score (ERS), outperforming traditional eplet mismatch assessments. Furthermore, T cell proliferation in mixed lymphocyte reaction in vitro correlates with the ERS, attenuated by antibody-mediated inhibition of a mismatched DSA-associated eplet. These results establish the differential immunological impacts of mismatched HLA eplets as integral in clinical practice and therapeutic innovation.
Keywords: DSA; HLA molecular mismatch; antibody-mediated rejection; eplet; risk score.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures






References
-
- Rodríguez-Perálvarez M., Germani G., Papastergiou V., Tsochatzis E., Thalassinos E., Luong T.V., Rolando N., Dhillon A.P., Patch D., O’Beirne J., et al. Early tacrolimus exposure after liver transplantation: relationship with moderate/severe acute rejection and long-term outcome. J. Hepatol. 2013;58:262–270. doi: 10.1016/j.jhep.2012.09.019. - DOI - PubMed
-
- Halloran P.F., Chang J., Famulski K., Hidalgo L.G., Salazar I.D.R., Merino Lopez M., Matas A., Picton M., de Freitas D., Bromberg J., et al. Disappearance of T Cell-Mediated Rejection Despite Continued Antibody-Mediated Rejection in Late Kidney Transplant Recipients. J. Am. Soc. Nephrol. 2015;26:1711–1720. doi: 10.1681/ASN.2014060588. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
