

A machine learning-derived angiogenesis signature for clinical prognosis and immunotherapy guidance in colon adenocarcinoma
- PMID: 40450107
- PMCID: PMC12126557
- DOI: 10.1038/s41598-025-03920-w
A machine learning-derived angiogenesis signature for clinical prognosis and immunotherapy guidance in colon adenocarcinoma
Abstract
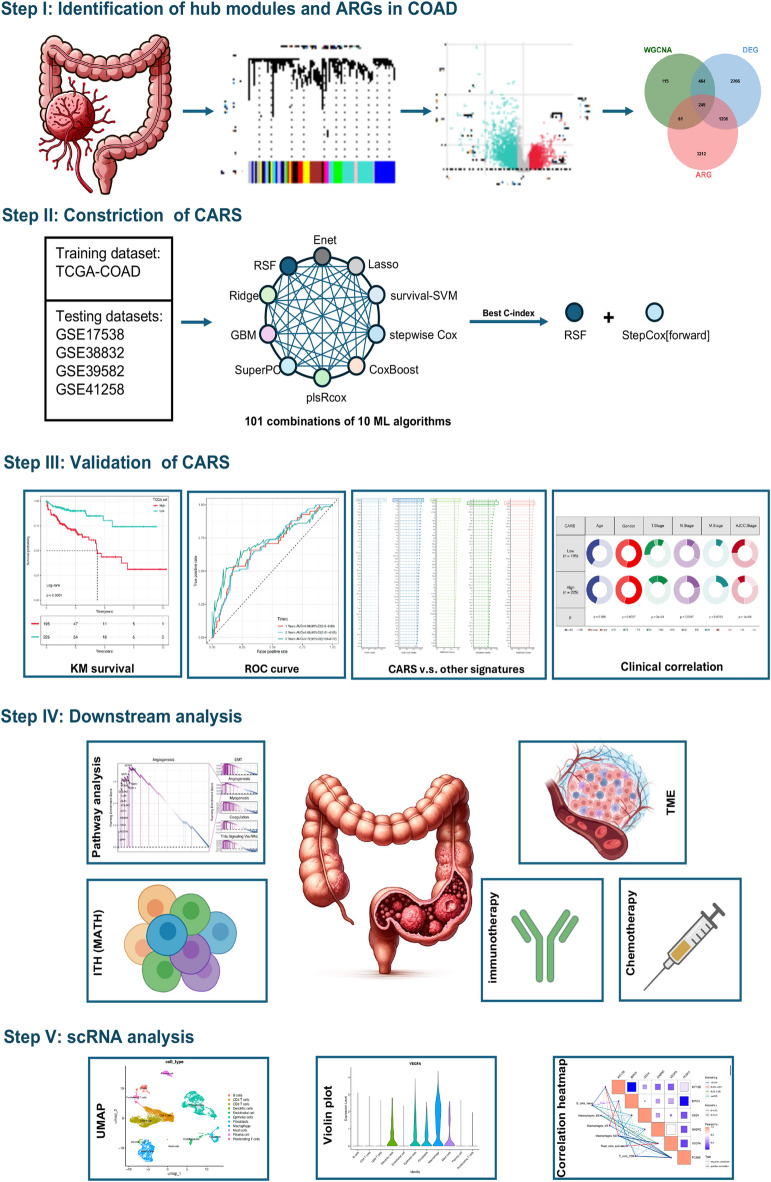
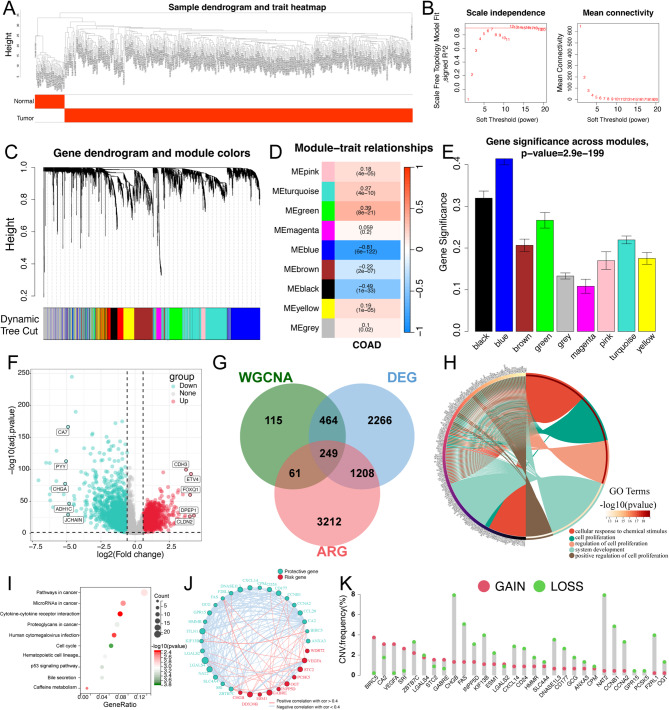
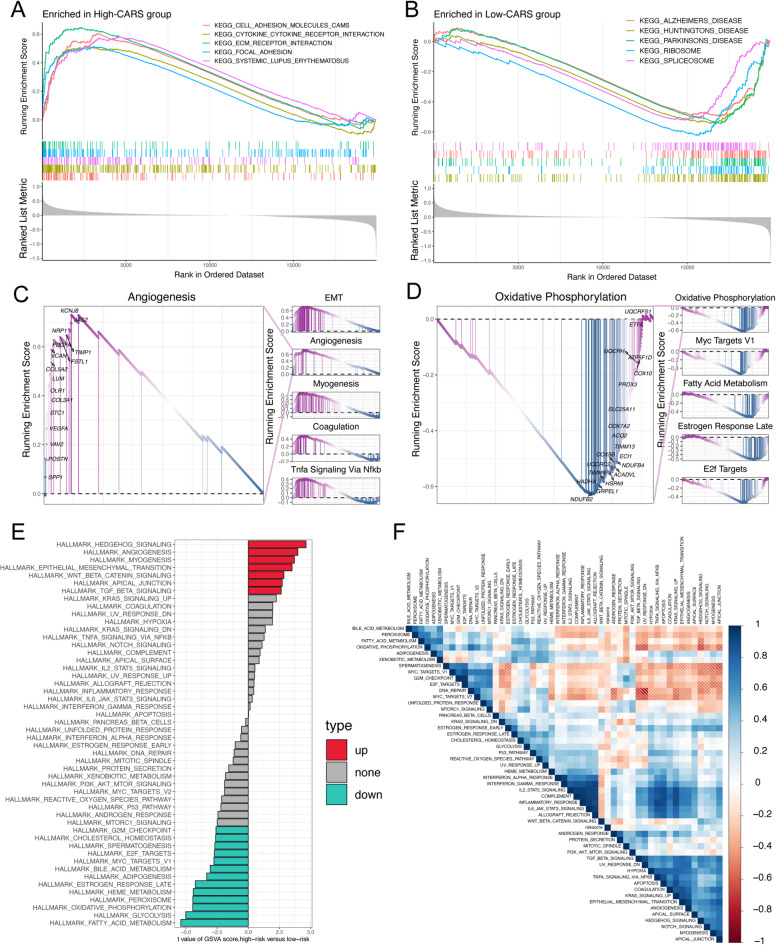
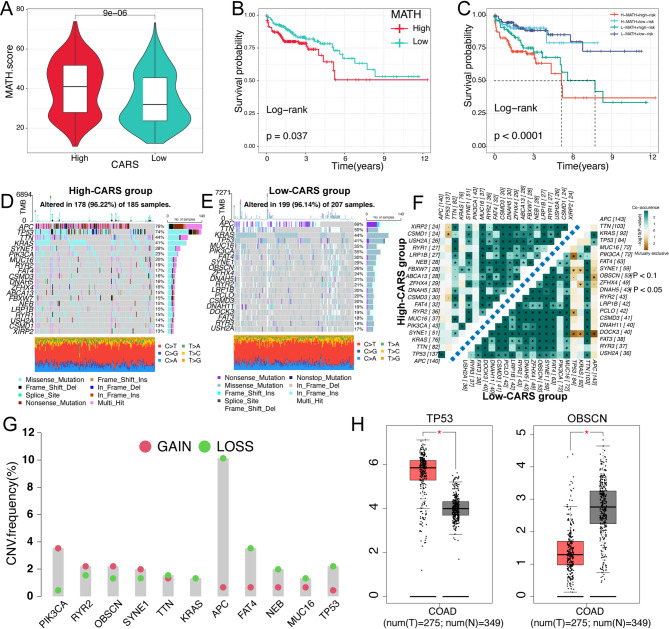
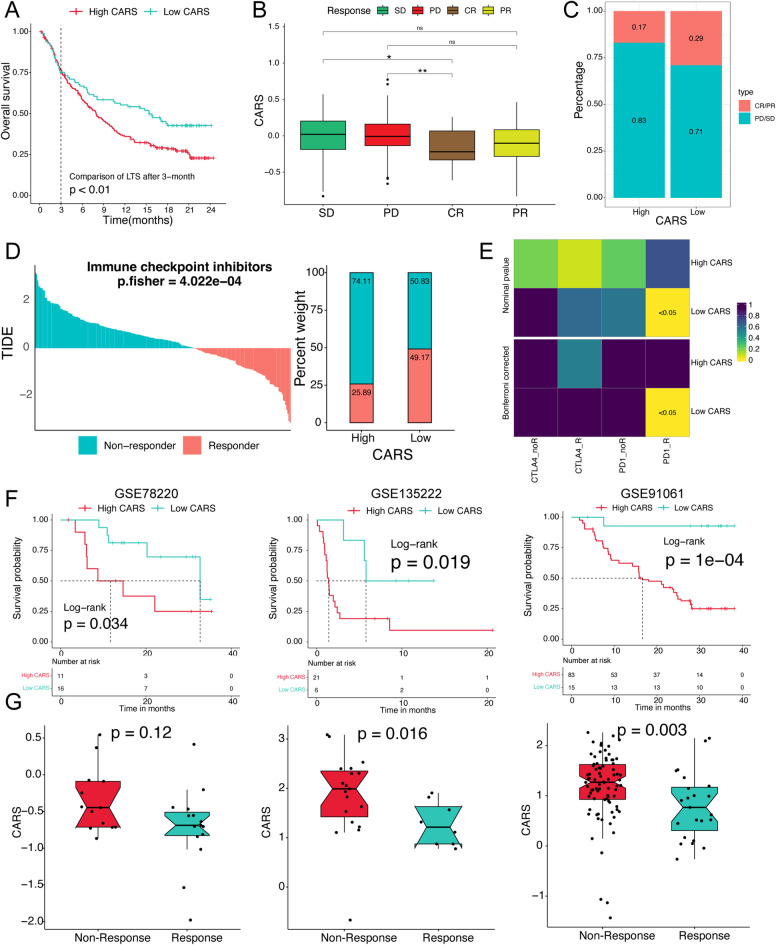
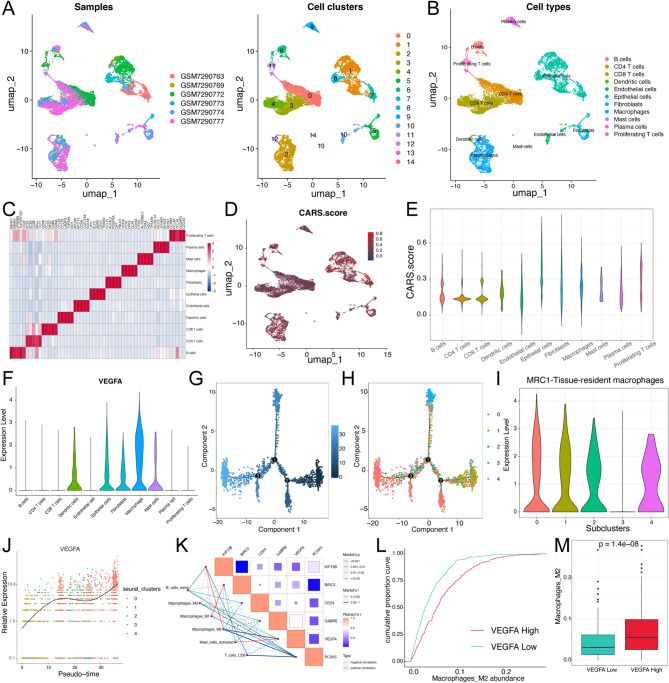
Colon adenocarcinoma (COAD) is one of the most prevalent malignancies worldwide and its prognosis is extremely poor. Angiogenesis has been linked to clinical outcomes, tumor progression, and treatment sensitivity. However, the role of angiogenesis in the COAD microenvironment and its interaction with immunotherapy remains unclear. In this study, an integrative machine learning approach, including ten algorithms, was used to construct a prognostic consensus angiogenesis-related signature (CARS) for COAD. The optimal CARS constructed using the RSF + StepCox [forward] algorithm had superior performance for clinical prognostic prediction and served as an independent risk predictor for COAD. Patients in the low-CARS group, characterized by immune activation, elevated tumor mutation/neoantigen burden, and greater responsiveness to immunotherapy, had a superior prognosis. Patients in the high-CARS group exhibited a poor prognosis with higher angiogenesis activity and immunosuppressive status, indicating lower immunotherapy benefits. However, axitinib and olaparib may be promising treatment options for such patients. Taken together, we constructed a prognostic CARS that provides prognostic stratification and elucidates the characteristics of the tumor microenvironment, which might guide the selection of personalized treatments for patients with COAD.
Keywords: Angiogenesis; Colon adenocarcinoma; Immunotherapy; Machine learning; Single cell RNA-seq; Tumor microenvironment.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures




References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
