

Perioperative durvalumab plus chemotherapy plus new agents for resectable non-small-cell lung cancer: the platform phase 2 NeoCOAST-2 trial
- PMID: 40450142
- PMCID: PMC12353838
- DOI: 10.1038/s41591-025-03746-z
Perioperative durvalumab plus chemotherapy plus new agents for resectable non-small-cell lung cancer: the platform phase 2 NeoCOAST-2 trial
Abstract
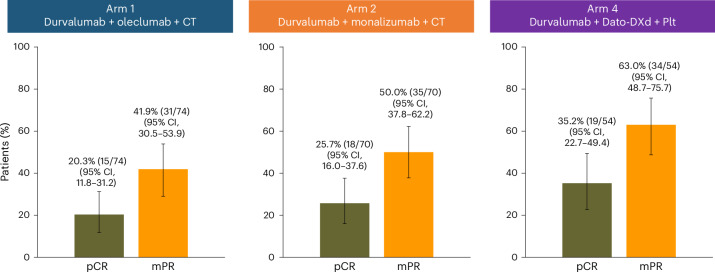
In the phase II NeoCOAST-2 platform study, 202 patients with untreated, resectable stage IIA-IIIB non-small-cell lung cancer (NSCLC) were randomized to receive neoadjuvant durvalumab plus platinum-doublet chemotherapy with oleclumab, a CD73 inhibitor (Arm 1), or with monalizumab, a NKG2A inhibitor (Arm 2), or neoadjuvant durvalumab plus single-agent platinum chemotherapy with the TROP-2 antibody-drug conjugate (ADC) datopotamab deruxtecan (Arm 4), followed by surgical resection and adjuvant durvalumab with oleclumab or monalizumab (Arms 1 and 2) or durvalumab alone (Arm 4). Primary endpoints were pathological complete response (pCR) rate and safety; secondary endpoints included feasibility of surgery and major pathological response (mPR) rate. In the modified intention-to-treat population (n = 198; Arm 1, n = 74; Arm 2, n = 70; Arm 4, n = 54), pCR rates were 20.3% (15/74; 95% CI, 11.8-31.2), 25.7% (18/70; 95% CI, 16.0-37.6) and 35.2% (19/54; 95% CI, 22.7-49.4), and mPR rates were 41.9% (31/74; 95% CI, 30.5-53.9), 50.0% (35/70; 95% CI, 37.8-62.2) and 63.0% (34/54; 95% CI, 48.7-75.7) in arms 1, 2, and 4, respectively. In the safety population, 69/74 (93.2%), 66/71 (93.0%), and 51/54 (94.4%) patients underwent surgery, respectively. Overall, grade ≥3 treatment-related adverse events occurred in 27/74 (36.5%), 29/71 (40.8%) and 11/54 (20.4%) patients, respectively. In NeoCOAST-2, the first neoadjuvant trial examining an ADC plus chemo-immunotherapy in resectable NSCLC, pCR rates were highest in the datopotamab-deruxtecan-containing arm, warranting further investigation in larger trials of ADCs and checkpoint inhibition in the neoadjuvant setting. ClinicalTrials.gov identifier: NCT05061550 .
© 2025. The Author(s).
Conflict of interest statement
Competing interests: T. C. has received over the past 24 months: speaker fees/honoraria (including travel/meeting expenses) from ASCO Post, AstraZeneca, Bio Ascend, Bristol Myers Squibb, Clinical Care Options, IDEOlogy Health, Medical Educator Consortium, Medscape, OncLive, PEAK Medicals, PeerView, Physicians’ Education Resource, Targeted Oncology; advisory role/consulting fees (including travel/meeting expenses) from AstraZeneca, Bristol Myers Squibb, Daiichi Sankyo, Genentech, Merck, Nuvalent, oNKo-innate, Pfizer, RAPT Therapeutics and Summit Therapeutics; and institutional research funding from AstraZeneca, Bristol Myers Squibb and Merck. L.B. reports speaker fees from and serving on the advisory board of MSD, BMS, Roche, Lilly, Takeda, Pfizer, Astra-Zeneca; institutional support from AstraZeneca; principal investigator of GCP trials for AstraZeneca, MSD, BMS, Roche, Pharmamar, Gilead, and Ose Immunotherapeutics. F. G. reports honoraria from Amgen, AstraZeneca, BMS, Johson, MSD, Pfizer, Regeneron, Roche, Sanofi, Takeda, Viatris; grants from Johnson & Johnson, Roche, Takeda. A.I. reports consulting fees from BeiGene, Roche, Takeda, MSD, Pfizer. O.B. reports honoraria from MSD, AstraZeneca, BMS; support for congress attendance from MSD, AstraZeneca, Takeda, Pfizer. R.C. reports honoraria and congress invitations from AstraZeneca. D.W.K. reports institutional funding from Alpha Biopharma, Amgen, AstraZeneca, BMS, Boehringer-Ingelheim, Bridge BioTherapeutics, Chong Keun Dang, Daiichi-Sankyo, GSK, Hanmi, IMBDx, InnoN, IQVIA, Janssen, Merck, Merus, Mirati Therapeutics, MSD, Novartis, ONO Pharmaceutical, Pfizer, Roche/Genentech, Takeda, TP Therapeutics, Xcovery, Yuhan; and medical writing assistance from Amgen, AstraZeneca, BMS, Boehringer-Ingelheim, Bridge BioTherapeutics, Chong Keun Dang, Daiichi-Sankyo, GSK, IMBDx, Janssen, Merus, Mirati Therapeutics, MSD, Meck, Novartis, Pfizer, Roche, Takeda, Yuhan. M.R.G.C. reports consulting fees and honoraria from Amgen, AstraZeneca, Bayer, Bristol Myers Squibb, Boehringer Ingelheim, F. Hoffmann-La Roche, Janssen, Lilly, MSD, Pfizer, Sanofi and Takeda. M.P.P. reports employment with Hospital Universitario Puerta de Hierro Universidad Autónoma de Madrid; serving on advisory councils for Amgen, Pfizer, Daiichi Sankyo, Johnson & Johnson, BMS, Takeda, AstraZeneca, Gilead, MSD, Guardant Health, Ipsen, Incyte Biosciences, Bayer; board of directors membership at the Instituto Investigación Sanitaria Puerta de Hierro Segovia de Arana, Grupo Español de Cáncer de Pulmón (Grupo Espñaol de Cáncer de Pulmón), Grupo Oncológico para el Tratamiento de las Enfermedades Linfoides (Spanish Lymphoma Oncology Group); honoraria from BMS, AstraZeneca, MSD, Roche, Takeda, Eli Lilly, F.Hoffman-La Roche, Janssen, Pfizer, Amgen; consulting fees from BMS, AstraZeneca, MSD, Roche, Takeda, Eli Lilly, F.Hoffman-La Roche, Janssen, Pfizer, Amgen; research funding from BMS, AstraZeneca, MSD, Roche, Takeda, Pfizer, Takeda, Boehringer Ingelheim, Amgen, Instituto de Salud Carlos III, Spanish Ministry of Science and Innovation, European Commission, Eli Lilly, F. Hoffmann-La Roche, Janssen, Pierre Fabre Pharmaceuticals. B.Y.S. reports advisory council for Guardant Health; grants from Yuhan. G. Metro reports advisory council for Amgen, Takeda, Daichii-Sankyo, Regeneron; consulting fees from Amgen, Daichii-Sankyo, Regeneron. J.B. reports serving on advisory councils or committees for AstraZeneca, Daiichi Sankyo, MSD, Johnson & Johnson; and honoraria from AstraZeneca, Bayer, Bristol Myers Squibb, Merck, MSD, Daiichi, Servier, Ipsen, Pierre Fabre Oncologie, Regeneron, Johnson & Johnson. A.B., A.Y., Y.H., A.D., G.K., R.K. and I.G. report employment and stock with AstraZeneca. LM. reports employment and stock with AstraZeneca; patent and patent applications with Gilead Sciences, Jounce Therapeutics, AstraZeneca. M.L., L.L. and T.E. report no conflicts of interest. J.S. reports having advisory and consultancy roles at AstraZeneca, Bristol Myers Squibb, Merck, Roche, Amgen, Chemocentryx, Xenetic Biosciences, Protalix Biotherapeutics, Novartis, Regeneron; contracted institutional grant and research support from AstraZeneca, Bristol Myers Squibb, Roche, Merck, CLS Therapeutics, Protalix Biotherapeutics; and speaker fees from PeerView, Bristol Myers Squibb, AstraZeneca and Merck. P.M.F. reports consulting fees from Ascendis, Amgen, AstraZeneca, BioNTech, BMS, Curevac, Novartis, Regeneron, G1, Genelux, Genentech, Gritstone, Merck, Janssen, F Star, Sanofi, Amgen, Fosun, Teva, Synthekine, Flame, Iteos, Tavotek, Teva; and grants and funding from AstraZeneca and BMS.
Figures





References
-
- American Cancer Society. Cancer Facts and Figures 2025 (ACS, 2025).
-
- Centers for Disease Control and Prevention. U.S. cancer statistics lung cancer stat bite (US Department of Health and Human Services, 2024); https://www.cdc.gov/united-states-cancer-statistics/publications/lung-ca...
-
- Baum, P. et al. An international registry study of early-Stage NSCLC treatment variations (LUCAEUROPE) in Europe and the USA highlighting variations. Eur. J. Cancer209, 114233 (2024). - PubMed
-
- Howington, J. A., Blum, M. G., Chang, A. C., Balekian, A. A. & Murthy, S. C. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest143, e278S–e313S (2013). - PubMed
-
- Goldstraw, P. et al. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J. Thorac. Oncol.11, 39–51 (2016). - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
