

Effectiveness of office hysteroscopy for retained products of conception: insights from 468 cases
- PMID: 40450188
- PMCID: PMC12374857
- DOI: 10.1007/s00404-025-08075-7
Effectiveness of office hysteroscopy for retained products of conception: insights from 468 cases
Abstract
Purpose: Retained products of conception (RPOC) are a common complication following pregnancy. Office hysteroscopy (OH) is increasingly used for diagnostics and management due to its minimally invasive nature. However, incidence of incomplete OH removal and procedures in which no RPOC are identified despite prior suspicion remains a concern. This study aimed to identify factors associated with these outcomes to improve patient selection and procedural success.
Methods: A retrospective study was conducted on patients referred for OH for presumed RPOC between August 2015 and April 2023 at the Department of Gynecology and Obstetrics, University Medical Centre Ljubljana, Slovenia. Inclusion criteria included hemodynamically stable patients with prolonged bleeding and/or suspicious ultrasound (US) findings post-pregnancy. Patients with RPOC thickness of more than 30 mm or strong tissue vascularization on US were excluded. Data on patient demographics, US features, and procedural outcomes were analyzed.
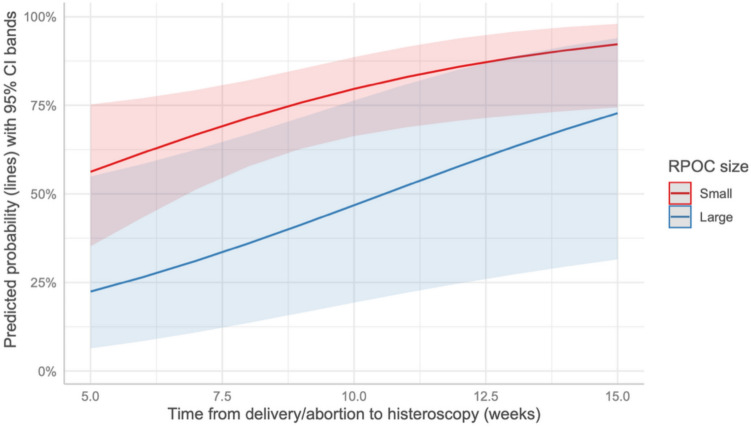
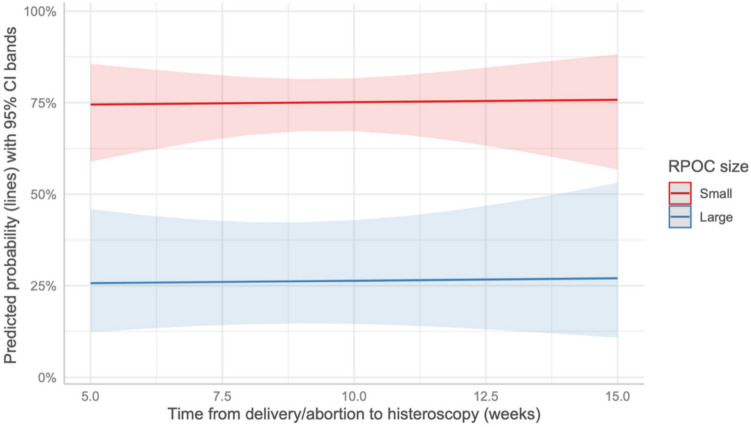
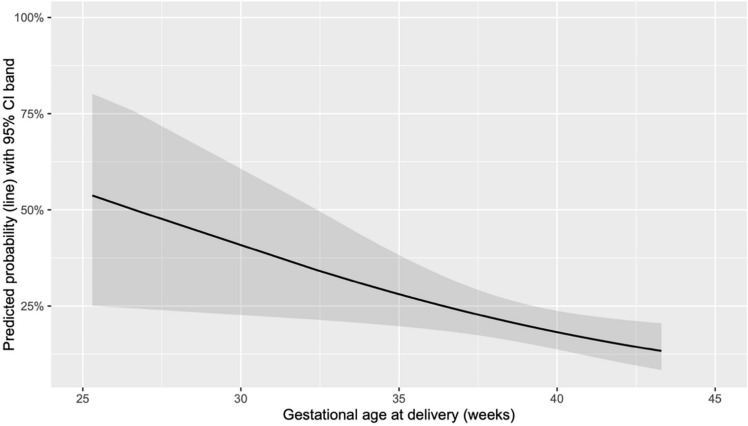
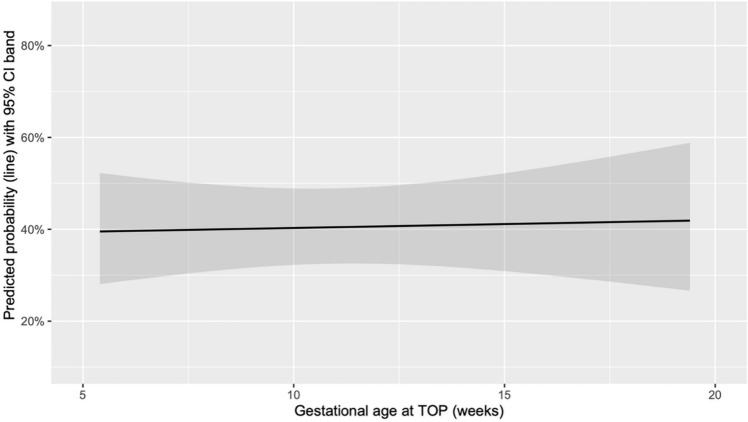
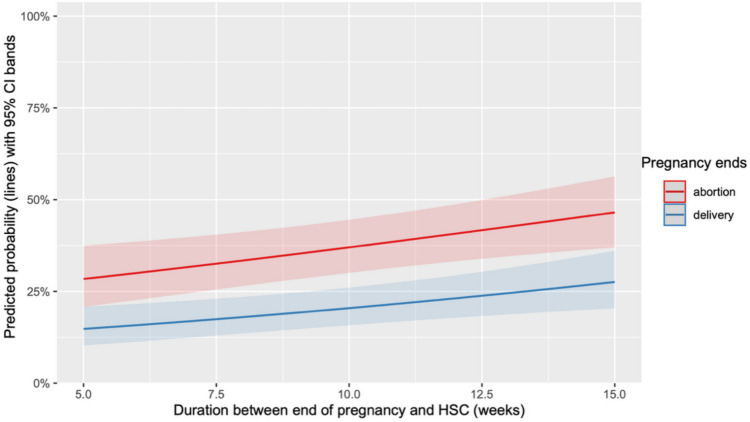
Results: Out of the 468 patients, RPOC removal was performed in 333 cases (71.2%), of which 225 (67.6%) were successfully completed, while in 135 cases (28.8%), the procedure was only diagnostic due to the absence of RPOC. Regarding procedural success, neither the pregnancy outcome, i.e., termination of pregnancy (TOP) vs delivery, nor gestational age significantly correlated with it. Longer time from pregnancy end to OH significantly improved procedural success in both groups, after TOP (p = 0.025) and in cases of large RPOC after delivery (p < 0.001). Parity significantly altered procedural success only in the delivery group (p < 0.007). The success rate of the procedure was significantly higher in cases when only small RPOC were observed (p < 0.001). Absence of RPOC occurred more frequently following TOP than after delivery (p < 0.001). Procedures in which no RPOC were confirmed were significantly associated with a longer interval between pregnancy end and OH in both TOP (p = 0.013) and delivery group (p = 0.003). Gestational age significantly correlated with the absence of RPOC only in the delivery group (p = 0.003). The likelihood of not confirming RPOC was higher where US thickness and length were lower (p = 0.007 and p = 0.011, respectively).
Conclusion: OH is effective for managing RPOC with a high success rate, but the absence of RPOC in a considerable number of OH-treated patients stresses the need for better diagnostic criteria and patient selection to minimize overtreatments. Further prospective studies are needed to optimize the timing and indications for OH.
Keywords: Minimally invasive surgery; Office hysteroscopy; Retained products of conception; Uterine diseases.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests. Ethical approval: The study was approved by the Republic of Slovenia National Medical Ethics Committee on 17.10.2023 (approval number: 0120-265/2023/3) and conducted in accordance with the principles of the Declaration of Helsinki. Consent to participate: Informed consent was obtained from all individuals included in the study. Consent for publication: Informed consent was obtained from all individuals included in the study.
Figures
References
-
- Westendorp IC, Ankum WM, Mol BW, Vonk J (1998) Prevalence of Asherman’s syndrome after secondary removal of placental remnants or a repeat curettage for incomplete abortion. Hum Reprod. 13:3347–50 - PubMed
-
- Smorgick N, Barel O, Fuchs N, Ben-Ami I, Pansky M, Vaknin Z (2014) Hysteroscopic management of retained products of conception: meta-analysis and literature review. Eur J Obstet Gynecol Reprod Biol. 173:19–22 - PubMed
-
- Hamerlynck TW, Blikkendaal MD, Schoot BC et al (2013) An alternative approach for removal of placental remnants: hysteroscopic morcellation. J Minim Invasive Gynecol. 20(6):796–802 - PubMed
-
- Achiron R, Goldenberg M, Lipitz S, Mashiach S (1993) Transvaginal duplex Doppler ultrasonography in bleeding patients suspected of having residual trophoblastic tissue. Obstet Gynecol. 81(4):507–11 - PubMed
-
- Alcázar JL (1998) Transvaginal ultrasonography combined with color velocity imaging and pulsed Doppler to detect residual trophoblastic tissue. Ultrasound Obstet Gynecol. 11(1):54–8 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
