

Analysis of clinical characteristics, treatment response, and prognosis among 67 patients with anaplastic multiple myeloma
- PMID: 40450260
- PMCID: PMC12126908
- DOI: 10.1186/s12957-025-03851-w
Analysis of clinical characteristics, treatment response, and prognosis among 67 patients with anaplastic multiple myeloma
Abstract
Background: Anaplastic multiple myeloma (AMM) is a type of distinctive MM with a poor prognosis. AMM is mostly reported as individual cases, an accurate incidence and strict clinical definition are lacking.
Methods: Sixty-seven patients with AMM were identified and then analyzed in the clinical database of patients with MM from January 2017 to September 2024.
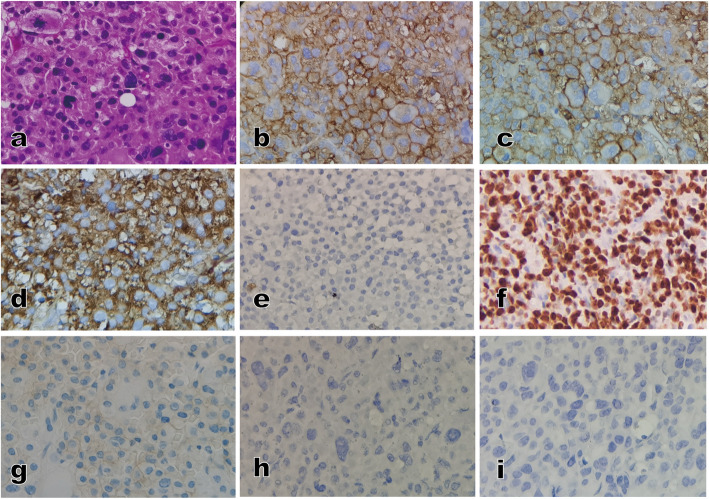
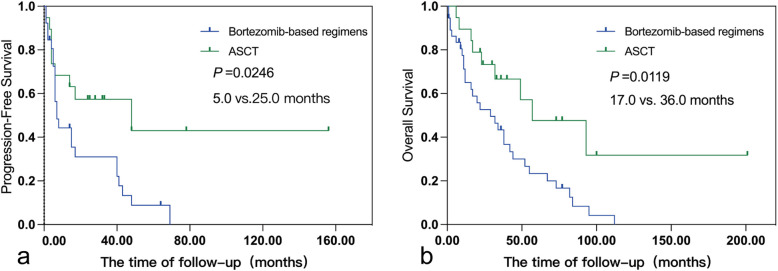
Results: The incidence of AMM among patients with MM was 3.3%. The IgD type accounted for 11.9% of patients, with 40.3% and 53.7% kappa and lambda light chains, respectively. Plasmablasts with larger diameters and multinuclear variations accounted for 46.7% from bone marrow or extramedullary disease (EMD) based on pathologic morphology; the average Ki-67 was 64.8%. The incidence of EMD was 49.3%. Lactic dehydrogenase (LDH) was elevated in 44.8% of patients and 49.3% of patients were International Staging System (ISS) III. The frequencies of 1q21, t (4; 14), and t (14; 16) in high-risk genes were 60.5%, 39.5%, and 18.4%, respectively. Double and triple gene hits were detected in 36.8% and 13.2% of patients, respectively. Fifty-six patients received treatment with bortezomib-based regimens. The progression-free survival (PFS) and overall survival (OS) of AMM patients in the autologous stem cell transplantation (ASCT) group were prolonged compared to patients who did not undergo ASCT with a median PFS and OS of 5.0 versus 25.0 and 17.0 versus 36.0 months, respectively (P = 0.0246 and P = 0.0119, respectively). At the time of the last follow-up, 71.4% of patients had died with 77.5% experiencing disease progression. A high neutrophil-to-lymphocyte ratio (NLR) and no ASCT were also independent prognostic factors for AMM patients.
Conclusions: The incidence of AMM is rare. The characteristics of these AMM patients included extensive proliferation of plasmablasts and widespread EMD formation, AMM patients also exhibit more invasive clinical manifestations and a short survival. Patients who underwent sequential ASCT after receiving bortezomib-based regimens partially overcame the poor prognosis of AMM.
Keywords: Anaplastic multiple myeloma; Clinical characteristics; Prognosis; Treatment response.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study has been approved by the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University (Ethics Approval Number: 2021-ke-516–1) and has obtained informed written consent from all patients and healthy individuals. Also,this study complies with the Helsinki Declaration and adheres to the principles of honest and rigorous clinical practice. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures




Similar articles
-
IgD multiple myeloma a descriptive report of 17 cases: survival and response to therapy.J Exp Clin Cancer Res. 2012 Mar 1;31(1):17. doi: 10.1186/1756-9966-31-17. J Exp Clin Cancer Res. 2012. PMID: 22381082 Free PMC article.
-
[Effects of extramedullary disease on patients with newly diagnosed multiple myeloma].Zhonghua Xue Ye Xue Za Zhi. 2023 Jan 14;44(1):48-54. doi: 10.3760/cma.j.issn.0253-2727.2023.01.009. Zhonghua Xue Ye Xue Za Zhi. 2023. PMID: 36987723 Free PMC article. Chinese.
-
LDH is an adverse prognostic factor independent of ISS in transplant-eligible myeloma patients receiving bortezomib-based induction regimens.Eur J Haematol. 2015 Apr;94(4):330-5. doi: 10.1111/ejh.12434. Epub 2014 Oct 18. Eur J Haematol. 2015. PMID: 25135740
-
[Prognostic factors in newly diagnosed multiple myeloma patients with 1q21 amplification/gain treated with bortezomib-based regimens followed by autologous hematopoietic stem cell transplantation].Zhonghua Xue Ye Xue Za Zhi. 2018 Jun 14;39(6):496-500. doi: 10.3760/cma.j.issn.0253-2727.2018.06.012. Zhonghua Xue Ye Xue Za Zhi. 2018. PMID: 30032568 Free PMC article. Chinese.
-
Autologous Transplantation for Newly Diagnosed Multiple Myeloma in the Era of Novel Agent Induction: A Systematic Review and Meta-analysis.JAMA Oncol. 2018 Mar 1;4(3):343-350. doi: 10.1001/jamaoncol.2017.4600. JAMA Oncol. 2018. PMID: 29302684 Free PMC article.
References
-
- Greipp PR, Raymond NM, Kyle RA, O’Fallon WM. Multiple myeloma: significance of plasmablastic subtype in morphological classification. Blood. 1985;65:305–10. - PubMed
-
- Greipp PR, Leong T, Bennett JM, et al. Plasmablastic morphology–an independent prognostic factor with clinical and laboratory correlates: Eastern Cooperative Oncology Group (ECOG) myeloma trial E9486 report by the ECOG Myeloma Laboratory Group. Blood. 1998;91:2501–7. - PubMed
-
- Di Stasi M, Cavanna L, Paties C, Fornari F, Civardi G, Binelli F, Buscarini E, Buscarini L. Anaplastic myeloma as extramedullary relapse of multiple myeloma in remission. Case report and review of the literature. Acta Haematol. 1986;76(4):202–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
