

Increased malignancy risk in patients with lymphangioleiomyomatosis: findings from a Chinese cohort
- PMID: 40450294
- PMCID: PMC12126872
- DOI: 10.1186/s13023-025-03834-w
Increased malignancy risk in patients with lymphangioleiomyomatosis: findings from a Chinese cohort
Abstract
Background: Lymphangioleiomyomatosis (LAM) is a rare, low-grade neoplasm. Abnormal activation of the mammalian target of rapamycin (mTOR) pathway plays a critical role in LAM pathogenesis by promoting cell proliferation, which may increase susceptibility to malignancies in these patients. However, owing to the rarity of LAM, comprehensive data on the risk of malignancy in this population are limited.
Methods: We retrospectively analyzed 849 LAM patients who participated in the LAM-China Registry Study at Peking Union Medical College Hospital. We collected medical records of patients with malignant tumors and estimated the incidence of malignancy in the LAM-China cohort.
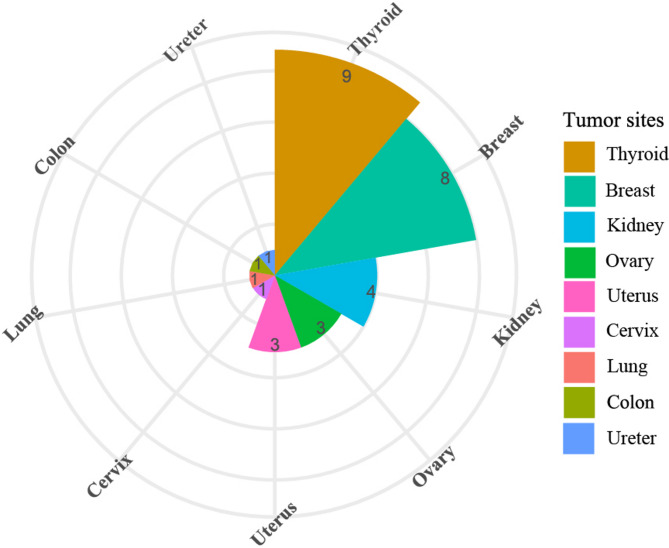
Results: A total of 849 patients were included in our research, of whom 760 were sporadic LAM and 89 had tuberous sclerosis complex-associated LAM. Thirty-one patients (3.65%) had a history of malignancy. More than 80% of LAM and malignant tumors developed successively within 5 years, with a median time interval of 1.5 years. Eighteen patients who were diagnosed with malignancy after diagnosis of LAM were included in the incidence calculation. The three most prevalent cancers were thyroid cancer (n = 5), breast cancer (n = 4) and ovarian cancer (n = 3). Except for lung cancer, the SIRs for all other cancers mentioned in the present study were significantly increased: thyroid cancer (SIR = 10.87, 95% CI 3.53-25.37), breast cancer (SIR = 5.95, 95% CI 1.62-15.24), and ovarian cancer (SIR = 24.54, 95% CI 5.07-71.86). After standardization by age, the SIR for malignancy in our cohort was 3.20 (95% CI 1.89-5.05, p = 0.00003). However, this elevated risk of malignancy appeared to be confined to younger age groups. Among individuals aged over 50 years, there was no statistically significant difference in the incidence of malignancy between LAM patients and the reference population.
Conclusion: The risk of malignant tumors is significantly increased in LAM patients than that in the reference population. Thyroid cancer, breast cancer, and ovarian cancer were the three most prevalent malignancies in our cohort. Each type of cancer that appeared in the cohort presented a relatively high incidence, except for lung cancer.
Keywords: Incidence; Lymphangioleiomyomatosis; Malignant tumor.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study is a subsidiary study of the LAM-Chian Registry Study. LAM-China was approved by the ethics committee of the Peking Union Medical College Hospital in Beijing (reference number JS-1323). Consent for publication: Signed informed consent was obtained from all participants. Competing interests: The authors declare that they have no competing interests. Statement: The abstract of this article has been accepted for POSTER presentation at the 2025 ATS International Conference. Currently, the relevant DOI and conference paper links have not been assigned.
Figures

References
-
- McCarthy C. Lymphangioleiomyomatosis: pathogenesis, clinical features, diagnosis, and management. Lancet Respiratory Med. 2021;1313–27. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
- 2022YFC2703901/National Key R&D Program of China
- U20A20341/National Natural Science Foundation of China
- 82170084/National Natural Science Foundation of China
- CIFMS 2021-I2M-1-003/the Chinese Academy of Medical Sciences (CAMS) Innovation Fund for Medical Sciences
- 2022-PUMCH-B-107/National High Level Hospital Clinical Research Funding
LinkOut - more resources
Full Text Sources
Miscellaneous
