

A Technique for Arthroscopic Double-Row Rotator Cuff Repair With Acellular Dermal Matrix Augmentation
- PMID: 40453022
- PMCID: PMC12126013
- DOI: 10.1016/j.eats.2024.103287
A Technique for Arthroscopic Double-Row Rotator Cuff Repair With Acellular Dermal Matrix Augmentation
Abstract
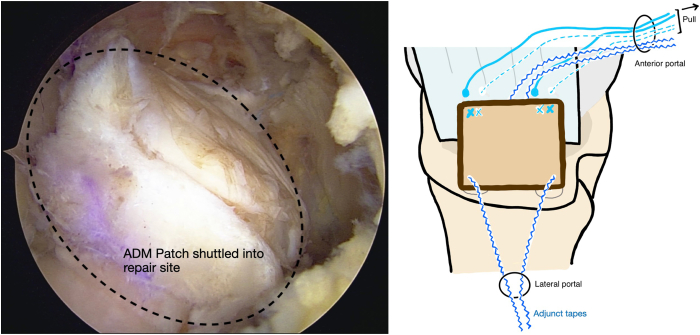
The outcomes of arthroscopic repair of large-to-massive rotator cuff tears remain suboptimal, with high retear rates reported. To overcome factors such as poor cuff quality and degenerate tendons with poor blood supply, augmentation with acellular dermal matrix allograft has emerged as a useful adjuvant procedure to promote healing. However, it remains a technically demanding procedure with a steep learning curve. Various described techniques require the use of additional suture anchors, tissue staples, or special instruments. This Technical Note describes a modified technique that streamline the steps and uses the standard 4 suture anchors for double-row cuff repair for the augmentation procedure.
© 2024 The Authors.
Figures













References
-
- Chung S.W., Oh J.H., Gong H.S., Kim J.Y., Kim S.H. Factors affecting rotator cuff healing after arthroscopic repair: osteoporosis as one of the independent risk factors. Am J Sports Med. 2011;39:2099–2107. - PubMed
-
- Tashjian R.Z., Hollins A.M., Kim H.-M., et al. Factors affecting healing rates after arthroscopic double-row rotator cuff repair. Am J Sports Med. 2010;38:2435–2442. - PubMed
LinkOut - more resources
Full Text Sources
