

doi: 10.1016/j.eats.2024.103318.
eCollection 2025 Apr.
Anatomic Medial Patellofemoral Ligament Reconstruction Using "Double-Socket" Technique
Affiliations
- PMID: 40453026
- PMCID: PMC12126022
- DOI: 10.1016/j.eats.2024.103318
Item in Clipboard
Anatomic Medial Patellofemoral Ligament Reconstruction Using "Double-Socket" Technique
Arthrosc Tech.
.
Abstract
In young individuals, recurrent patellar dislocation is a common issue. Surgical treatment often involves reconstructing the medial patellofemoral ligament. Various techniques exist, but most involve large transpatellar tunnels or suture anchors. Our medial patellofemoral ligament reconstruction technique uses 2 small sockets on the medial border of the patella. There are no implants in the patella, which reduces the risk of patellar fracture. The graft, which is already secured in these sockets, obtains additional attachment to the roughened medial patellar border, thereby promoting robust healing and stability. This approach is both effective and cost-efficient.
© 2024 The Authors.
Figures

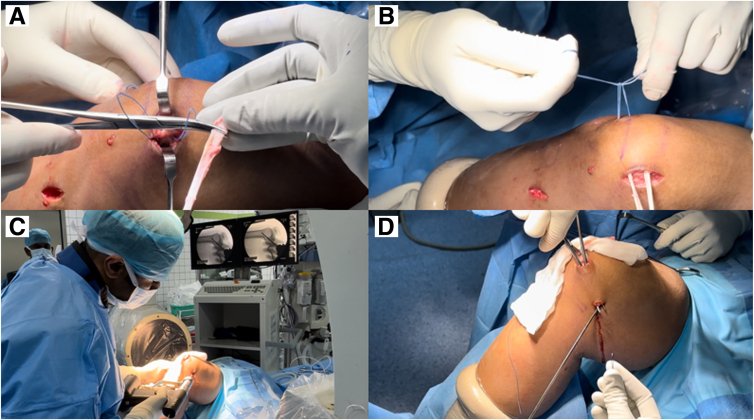
View from medial aspect of right knee held at 60° of flexion. (A) A longitudinal incision (approximately 3 cm in length) is made close to the medial border of the patella. Careful dissection is carried out to expose the medial border of the patella. (B) Two 2.4-mm Beath pins are passed from the medial to lateral aspect of the patella. The 2 pins should be at least 1 cm apart, and the lower pin should not cross over to the lower half of the patella. The surgeon should take care not to violate the articular surface of the patella by not directing the wire inferiorly. (C) The Beath pins are over-drilled with a 4.5-mm cannulated reamer to create 2 sockets of 15 mm in depth on the medial aspect of the patella. A depth of 15 mm may be marked over the cannulated reamer as well. (D) Two separate FiberWire are shuttled through the tunnels such that the loop ends come to the medial aspect of the patella and the free ends are on the patellar aspect of the patella.
View from medial aspect of right knee held at 60° of flexion. (A) The graft is passed through each of the FiberWire loops coming through from the medial border of the patella. Care should be taken to keep the midportion of the graft between the 2 loops. (B) Each of the FiberWire threads at the lateral border of the patella is pulled in such a way that a loop of graft becomes pulled into each of the 2 sockets. The FiberWire threads are then tied on the lateral aspect of the patella. The 2 free ends of the graft come out from the medial border of the patella. (C) The Schöttle point is identified under image guidance, and a guidewire is placed in the proximal and anterior direction to avoid iatrogenic damage to the trochlea (D) A soft-tissue tunnel is created from the medial border of the patella toward the adductor tubercle. The tunnel passes in the plane between layer 2 and layer 3 of the medial aspect of the knee.

View from medial aspect of right knee held at 60° of flexion. The 2 free ends of the graft are shuttled through the soft-tissue tunnel and whipstitched; then, sizing is carried out. An appropriately sized reamer is passed over the guide pin fixed at the Schöttle point, and reaming is performed. An interference screw (1 size larger than the graft size) is carefully inserted to complete femoral fixation. During screw insertion, an assistant holds the FiberWire threads (at the whipstitched femoral end of the graft) in mild tension.

Entire construct including sockets for MPFL reconstruction in the right knee. (1) FiberWire threads tied at lateral border of patella. These threads traverse the 2.4-mm transpatellar tunnels made from the medial to lateral aspect. (2) Looped graft inside superior socket. Each socket is 15 mm deep and 4.5 mm wide and is created by reaming the 2.4-mm transpatellar tunnel with a 4.5-mm cannulated reamer—but only to a depth of 15 mm. (3) Looped graft inside inferior socket. (4) Graft tissue spanning distance between 2 sockets, which is in contact with roughened medial patellar border. (5) Femoral fixation of free ends coming out from sockets after being whipstitched together.
References
LinkOut - more resources
Full Text Sources
