

Metagenomic Next-generation Sequencing Compared With Blood Culture as First-line Diagnostic Method for Bloodstream Infection in Hematologic Patients With Febrile Neutropenia: A Multicenter, Prospective Study
- PMID: 40453877
- PMCID: PMC12125677
- DOI: 10.1093/ofid/ofaf288
Metagenomic Next-generation Sequencing Compared With Blood Culture as First-line Diagnostic Method for Bloodstream Infection in Hematologic Patients With Febrile Neutropenia: A Multicenter, Prospective Study
Abstract
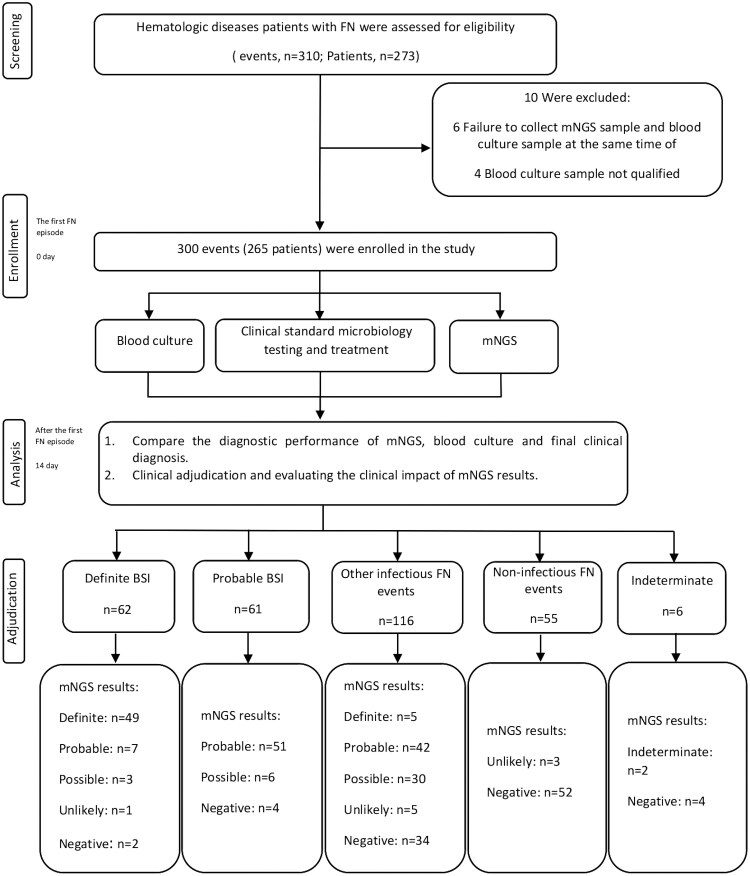
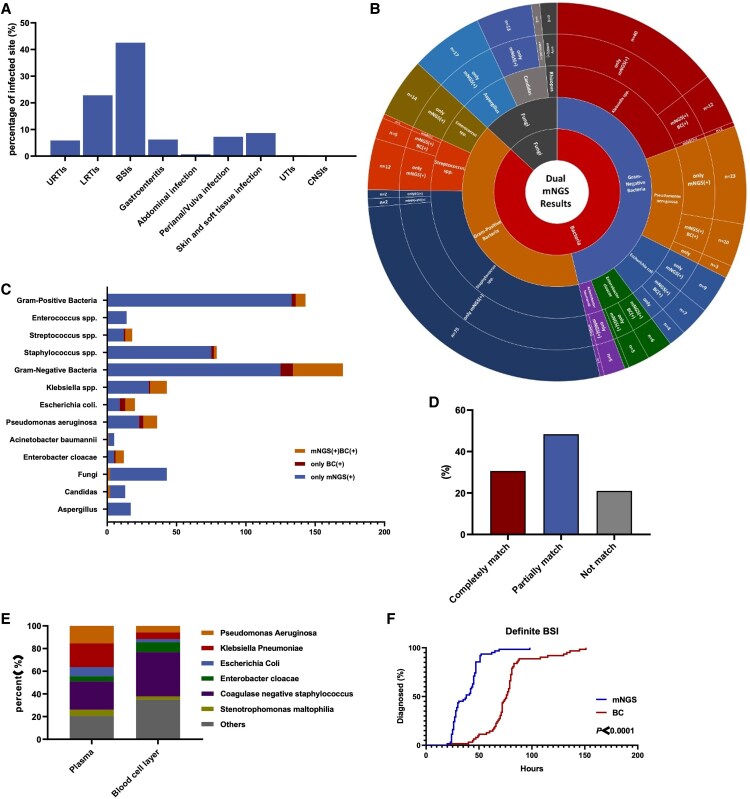
Bloodstream infection (BSI) is a frequent but lethal complication in hematologic patients with febrile neutropenia (FN). However, blood culture (BC) only detects an organism in 20%-30% of patients with FN. We aimed to evaluate the diagnostic performance of metagenomic next-generation sequencing (mNGS) as a first-line diagnostic method in BSI. This study was prospectively performed in 4 Chinese hematologic centers. In patients aged ≥15 years with hematologic diseases, peripheral blood specimens were collected per patient for simultaneous BC and mNGS at the onset of FN. The clinical physician and mNGS analysis team were double-blinded, and the adjudication of the clinical diagnosis was evaluated by another expert panel of 4 specialists. The primary endpoint of this study was the diagnostic performance of mNGS. This study was registered on ClinicalTrials.gov. Three hundred FN events were enrolled, including 62 definite BSI, 61 probable BSI, 116 infectious FN other than BSI, 55 noninfectious FN events, and 6 FN of indeterminate cause. Among 62 definite BSI cases, mNGS identified causative pathogens in 59 (95.2%). Concurrent BC initially detected pathogens in 59 cases, and 3 additional pathogens consistent with mNGS were later identified in repeated BC testing. The sensitivity, specificity, positive predictive value, and negative predictive value of mNGS were 95.2%, 94.6%, 95.2%, and 94.6%, respectively. The diagnostic time of mNGS was significantly shorter than that of BC (39.7 ± 15.0 vs 119.8 ± 31.9 hours, P < .0001). The findings suggest that the mNGS approach has excellent diagnostic performance for the first-line diagnosis of BSI in patients with FN. The study will promote early diagnosis and better management of the patients.
Keywords: blood culture; bloodstream infection; febrile neutropenia; hematologic diseases; mNGS.
© The Author(s) 2025. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts.
Figures
Similar articles
-
Clinical metagenomic sequencing of plasma microbial cell-free DNA for febrile neutropenia in patients with acute leukaemia.Clin Microbiol Infect. 2024 Jan;30(1):107-113. doi: 10.1016/j.cmi.2023.05.034. Epub 2023 Jun 2. Clin Microbiol Infect. 2024. PMID: 37271194
-
Pathogen Detection by Metagenomic Next-Generation Sequencing During Neutropenic Fever in Patients With Hematological Malignancies.Open Forum Infect Dis. 2022 Jul 30;9(8):ofac393. doi: 10.1093/ofid/ofac393. eCollection 2022 Aug. Open Forum Infect Dis. 2022. PMID: 36004313 Free PMC article.
-
Etiological diagnostic performance of probe capture-based targeted next-generation sequencing in bloodstream infection.J Thorac Dis. 2024 Apr 30;16(4):2539-2549. doi: 10.21037/jtd-24-400. Epub 2024 Apr 18. J Thorac Dis. 2024. PMID: 38738241 Free PMC article.
-
The Value of Metagenomic Next-Generation Sequencing in Hematological Malignancy Patients with Febrile Neutropenia After Empiric Antibiotic Treatment Failure.Infect Drug Resist. 2022 Jul 7;15:3549-3559. doi: 10.2147/IDR.S364525. eCollection 2022. Infect Drug Resist. 2022. PMID: 35837537 Free PMC article.
-
Blood plasma metagenomic next-generation sequencing for identifying pathogens of febrile neutropenia in acute leukemia patients.Sci Rep. 2023 Nov 20;13(1):20297. doi: 10.1038/s41598-023-47685-6. Sci Rep. 2023. PMID: 37985857 Free PMC article.
References
-
- Yan CH, Wang Y, Mo XD, et al. Incidence, risk factors, microbiology and outcomes of pre-engraftment bloodstream infection after haploidentical hematopoietic stem cell transplantation and comparison with HLA-identical sibling transplantation. Clin Infect Dis 2018; 67(Suppl 2):S162–73. - PubMed
-
- Klastersky J. Management of fever in neutropenic patients with different risks of complications. Clin Infect Dis 2004; 39(Suppl 1):S32–7. - PubMed
-
- Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis 2011; 52:427–31. - PubMed
-
- Feng S, Rao G, Wei X, et al. Clinical metagenomic sequencing of plasma microbial cell-free DNA for febrile neutropenia in patients with acute leukaemia. Clin Microbiol Infect 2024; 30:107–13. - PubMed
-
- Xu C, Chen X, Zhu G, et al. Utility of plasma cell-free DNA next-generation sequencing for diagnosis of infectious diseases in patients with hematological disorders. J Infect 2023; 86:14–23. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
