

Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis
- PMID: 40453921
- PMCID: PMC12126676
- DOI: 10.1177/20543581251331703
Lived Experiences of Sexual and Gender Minorities in Solid Organ Transplantation: A Best-Fit Framework Synthesis and Inductive Thematic Analysis
Abstract
Background: Organ and tissue donation and transplantation (OTDT) policies and practices lead to differential care for sexual and gender minorities (SGMs). The experiences of SGM patients and caregivers in the transplantation system have not been published. The perspectives of SGMs on how to best address existing inequities are not understood.
Objective: To characterize the lived experiences of SGM patients and caregivers in solid-organ transplant health systems, as well as the perspectives and priorities of these individuals regarding SGM-relevant policies, practices and targets for system improvements.
Methods: We conducted a series (N = 12) of one-on-one semi-structured interviews with a convenience sample of SGMs with lived experience of the OTDT system. We transcribed interviews verbatim and performed a formal qualitative analysis combining a best-fit framework synthesis and inductive thematic analysis.
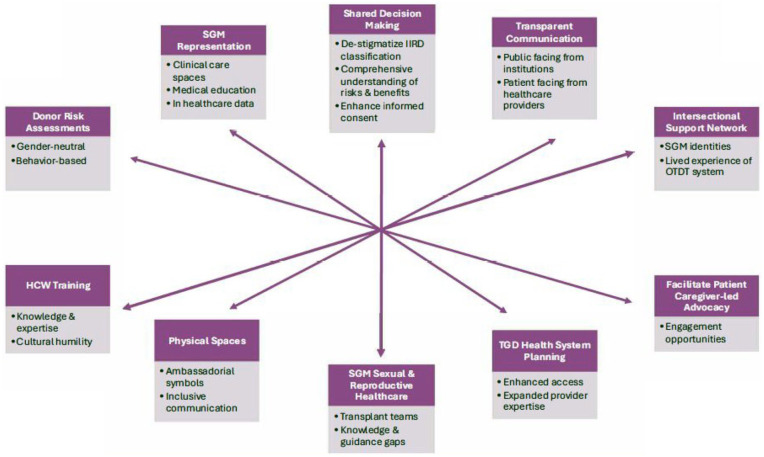
Results: We revealed novel targets for action to improve inclusive care in the transplantation system directly informed by the lived experiences of SGM patients and caregivers. Targets for improvement included (1) enhancements to shared decision-making between OTDT providers and patients, (2) transparent communication from OTDT organizations, (3) data-driven donor risk assessments, (4) expanded healthcare worker training, (5) inclusive physical care spaces, (6) recommendations for transgender and gender-diverse health system planning, (7) integrated sexual and reproductive healthcare services for transplant recipients, (8) increased SGM representation in medical education and care settings, (9) SGM and OTDT intersectional support networks, and (10) structural facilitation of SGM community advocacy efforts.
Limitations: While thematic saturation was achieved with our sample, we recognize that not all SGM identities were represented. It remains likely that additional experiences, beliefs, and priorities exist in the SGM community.
Conclusions: The emergent priorities and perspectives of SGMs with lived experience of transplant systems should inform patient-centered equitable health system advancements.
Contexte: Les politiques et pratiques actuelles entourant le don et la transplantation d’organes et de tissus (DTOT) entraînent des différences dans les soins des personnes membres de minorités sexuelles et de genre (MSG). Aucun article publié ne fait état des expériences des patients et soignants membres de MSG dans le système de transplantation. Le point de vue de ces personnes sur la meilleure façon de remédier à ces inégalités est encore mal connu.
Objectifs: Caractériser les expériences vécues par les patients et soignants membres de MSG dans les systèmes de transplantation d’organes solides, et connaitre leur point de vue et leurs priorités en matière de politiques, de pratiques et de cibles d’amélioration du système pertinentes pour les MSG.
Méthodologie: Nous avons mené une série d’interviews individuelles semi-structurées (n=12) auprès d’un échantillon de commodité composé de personnes membres de MSG ayant un vécu expérientiel du système de DTOT. Nous avons retranscrit textuellement le contenu des interviews et procédé à une analyze qualitative formelle combinant une synthèse du cadre le mieux adapté et une analyze thématique inductive.
Résultats: Nous avons mis en évidence de nouvelles cibles d’action, reposant directement sur le vécu expérientiel des patients et soignants membres de MSG, pour favoriser l’inclusion dans les soins du système de transplantation. Ces cibles étaient les suivantes : 1) amélioration de la prise de décision partagée entre les prestataires de soins de DTOT et les patients; 2) communications transparentes des organismes de DTOT; 3) évaluations des risques pour les donneurs fondées sur les données probantes; 4) élargissement de la formation du personnel de santé; 5) espaces plus inclusifs pour les soins physiques; 6) recommandations pour la planification dans le système de santé pour les personnes transgenres et la diversité des genres; 7) services intégrés de santé sexuelle et reproductive pour les receveurs d’une greffe; 8) représentation accrue des MGS dans l’enseignement médical et les structures de soins; 9) réseaux de soutien croisés entre les MSG et les systèmes de DTOT; 10) facilitation structurelle des efforts pour la défense des intérêts des communautés des MSG.
Limites: Bien que nous ayons atteint la saturation thématique avec notre échantillon, nous reconnaissons que toutes les identités des MSG n’étaient pas représentées. Il est possible que d’autres expériences, avis et priorités existent dans les différentes communautés des MSG.
Conclusion: Le point de vue et les priorités émergentes des membres des MSG ayant un vécu expérientiel des systèmes de transplantation devraient guider les progrès des systèmes de santé plus équitables et centrés sur le patient.
Keywords: donor risk assessments; donor-derived infections; equity; gender identity; inclusive care; organ and tissue donation and transplantation; safety; sexual and gender minorities; sexual orientation.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Sexual and gender minoritized persons in organ and tissue donation: a qualitative analysis.Can J Anaesth. 2025 Aug;72(8):1207-1219. doi: 10.1007/s12630-025-03011-4. Epub 2025 Jul 15. Can J Anaesth. 2025. PMID: 40665182 Free PMC article.
-
Sexual and gender minority relevant policies in Canadian and United States organ and tissue donation and transplantation systems: An opportunity to improve equity and safety.Am J Transplant. 2024 Jan;24(1):11-19. doi: 10.1016/j.ajt.2023.08.027. Epub 2023 Sep 1. Am J Transplant. 2024. PMID: 37659606
-
Improving Sexual and Gender Minority Cancer Care: Patient and Caregiver Perspectives From a Multi-Methods Pilot Study.Front Oncol. 2022 May 6;12:833195. doi: 10.3389/fonc.2022.833195. eCollection 2022. Front Oncol. 2022. PMID: 35600396 Free PMC article.
-
Culturally Competent Gender, Sex, and Sexual Orientation Information Practices and Electronic Health Records: Rapid Review.JMIR Med Inform. 2021 Feb 11;9(2):e25467. doi: 10.2196/25467. JMIR Med Inform. 2021. PMID: 33455901 Free PMC article. Review.
-
From patients to providers: changing the culture in medicine toward sexual and gender minorities.Acad Med. 2015 May;90(5):574-80. doi: 10.1097/ACM.0000000000000656. Acad Med. 2015. PMID: 25650825 Review.
References
-
- Ipsos. LGBT+ Pride 2021 global survey: a 27-country Ipsos survey. Published 2021. Accessed March 22, 2025. https://www.ipsos.com/en/lgbt-pride-2021-global-survey-points-generation...
LinkOut - more resources
Full Text Sources
