

Therapeutic time window of disease-modifying therapy for early Alzheimer's disease
- PMID: 40453977
- PMCID: PMC12122261
- DOI: 10.1002/trc2.70102
Therapeutic time window of disease-modifying therapy for early Alzheimer's disease
Abstract
Introduction: Recently approved disease-modifying therapies (DMT) for early Alzheimer's disease (AD), including lecanemab and donanemab, require patients to meet specific eligibility criteria for treatment. These criteria define a limited "therapeutic time window," after which patients become ineligible as the disease advances. Understanding factors influencing this window may help clinicians optimize patient management and reduce lost treatment opportunities.
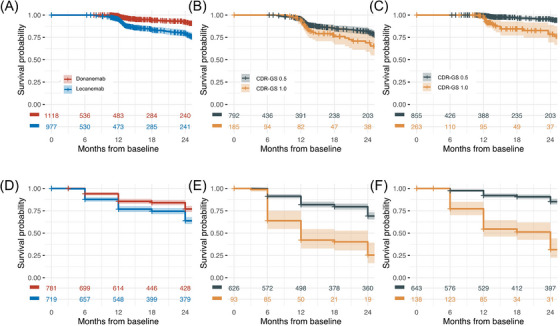
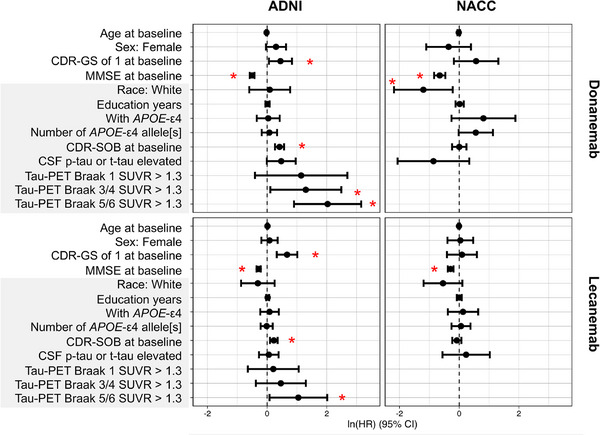
Methods: We analyzed longitudinal data from two observational cohorts, the National Alzheimer's Coordinating Center (NACC) and the Alzheimer's Disease Neuroimaging Initiative (ADNI). At each visit, individuals were deemed eligible if they were amyloid-positive and had a Mini-Mental State Examination (MMSE) score of 22-30 (lecanemab) or 20-30 (donanemab), plus a Clinical Dementia Rating-Global Score (CDR-GS) of 0.5 or 1. We then applied survival analyses and Cox proportional hazards models to estimate time-to-ineligibility based on baseline cognitive status.
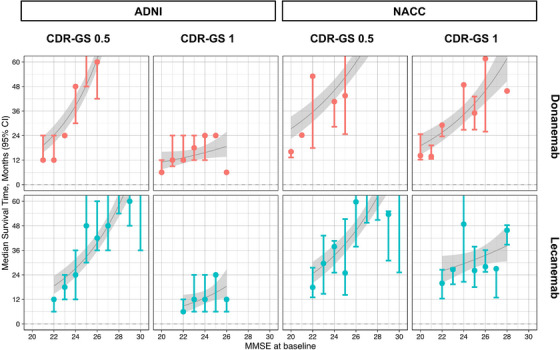
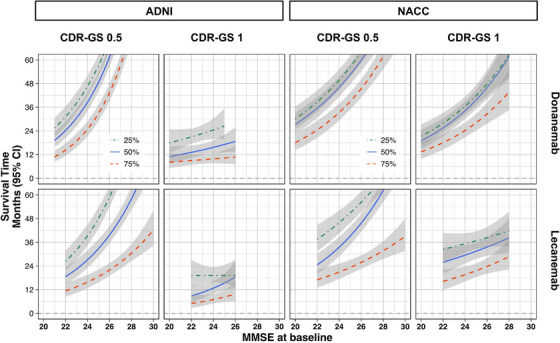
Results: Across both datasets, higher baseline CDR-GS and MMSE were associated with a lower risk of becoming ineligible (pooled hazard ratio of 1.601 for CDR-GS of 1 vs. 0.5, and pooled hazard ratio of 0.660 per 1-point increase in MMSE score above the lower limit of eligibility). The estimated 75% survival time for patients with baseline CDR-GS 0.5 was over 12 months, suggesting only 25% would become ineligible within 12 months. For those with CDR-GS 1, the estimated 50% survival time was approximately 12 months, depending on the data, indicating that half might become ineligible within 1 year.
Discussion: We quantitatively outlined the duration of the therapeutic time window for early AD patients who qualify for lecanemab or donanemab, which is significantly influenced by baseline CDR-GS and MMSE scores. These findings will support more proactive patient management, ensuring timely evaluations and prioritization of patients at higher risk of ineligibility, particularly where DMT access is limited.
Highlights: We examined the "therapeutic time window" eligibility for disease-modifying therapy.Longitudinal data from National Alzheimer's Coordinating Center (NACC) and Alzheimer's Disease Neuroimaging Initiative (ADNI) were used to quantify eligibility duration.Higher Clinical Dementia Rating-Global Score (CDR-GS) or lower Mini-Mental State Examination (MMSE) at baseline were associated with shorter window length.Our results will help optimize the management of the wait time for disease-modifying therapies (DMT) treatment.
Keywords: ADNI; Alzheimer's disease; NACC; disease‐modifying therapy; therapeutic window.
© 2025 The Author(s). Alzheimer's & Dementia: Translational Research & Clinical Interventions published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
The authors have no conflict of interest to disclose. Author disclosures are available in the Supporting Information.
Figures
References
-
- van Dyck CH, Sabbagh M, Cohen S. Lecanemab in early Alzheimer's disease. reply. N Engl J Med. 2023;388(17):1631‐1632. - PubMed
-
- Gil DR. Donanemab: Appropriate Use Recommendations. In: 17th Clinical Trials in Alzheimer's Disease Conference , October 30. Journal of Prevention of Alzheimer's Disease; 2024.
-
- Ministry of Health, Labour, and Welfare . LEQEMBI Optimal Use Guideline [Article in Japanese]. Accessed on Dec 13, 2023 (https://www.mhlw.go.jp/content/12404000/001178607.pdf):
LinkOut - more resources
Full Text Sources