

Comparison of NADAL COVID IgG/IgM rapid test and DiaSorin Liaison SARS-CoV-2 S1/S2 IgG assay across different blood sources and substrates
- PMID: 40454936
- PMCID: PMC12211023
- DOI: 10.1128/spectrum.03350-24
Comparison of NADAL COVID IgG/IgM rapid test and DiaSorin Liaison SARS-CoV-2 S1/S2 IgG assay across different blood sources and substrates
Abstract
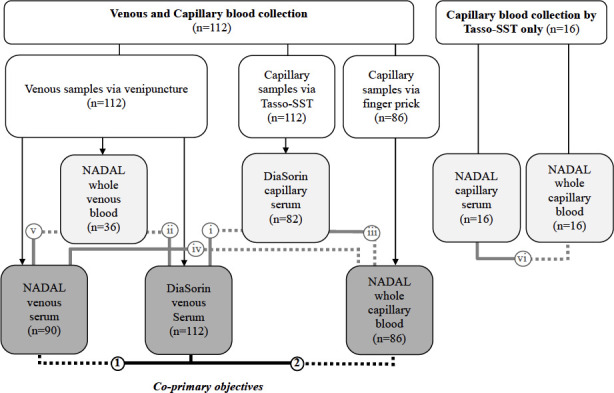
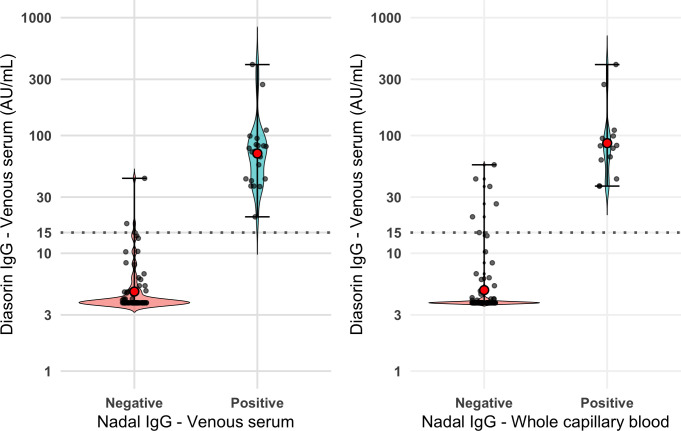
The NADAL COVID-19 IgG/IgM (NADAL) assay, approved for rapid testing on serum or plasma, had not been approved nor tested as a point-of-care test on capillary blood. The study aim was to evaluate the performance of NADAL compared to that of the DiaSorin Liaison SARS-CoV-2 S1/S2 IgG (DiaSorin) assay (gold standard). We conducted two cross-sectional studies in participants aged ≥2 years, in whom different blood substrates (whole blood vs serum) and sources (venous vs capillary) were sampled. The co-primary endpoints were agreement in IgG detection between NADAL on venous serum and whole capillary blood vs DiaSorin on venous serum. Among 128 participants, 23.2% had a positive DiaSorin IgG assay. The NADAL IgG on venous serum exhibited near-perfect agreement (κ = 0.91) and high accuracy (0.94, 95% CI: 0.87-1.00), with a sensitivity of 0.88 and perfect specificity compared to DiaSorin; NADAL IgG on whole capillary blood exhibited moderate agreement (κ = 0.77) and accuracy (0.84, 95% CI: 0.73-0.95), with a sensitivity of 0.68 and perfect specificity. As for secondary outcomes, when the two assays were compared within the same source (venous or capillary) but with different substrates (NADAL on whole blood vs DiaSorin on serum), strong agreement and high accuracy were observed. Within-test DiaSorin IgG assay on capillary vs venous serum showed near-perfect agreement and high accuracy. Within-test NADAL IgG assays on whole capillary blood vs capillary or venous serum demonstrated high accuracy. In conclusion, NADAL on venous serum exhibited near-perfect agreement and high accuracy with DiaSorin on venous serum but lower between-test performance on different blood substrates.
Importance: Accurate serological assays are essential for assessing population immunity levels and identifying vulnerable subgroups with lower immunity on which to focus vaccination efforts. Although rapid tests may offer the possibility of easy point-of-care testing on whole capillary blood for these purposes, they may not be as robust as other assays when used on different blood substrates or sources than those in which they were approved. The observed variability in test performance across different substrates and blood sources highlights the importance of pretesting assays under the specific conditions in which they would be used to ensure optimal interpretation of the immune status in the community.
Keywords: NADAL COVID-19 Test; SARS-CoV-2 IgG/IgM serology; diagnostic accuracy; point-of-care testing; sensitivity and specificity; whole capillary blood.
Conflict of interest statement
F.M.D. has received unrestricted research funds from AstraZeneca, Covis Pharma, GlaxoSmithKline, Merck Canada, Novartis, Teva, Trudell Medical, GlaxoSmithKline, and MEDteq in partnership with Thorasys Inc.; an honorarium for consultancy work from AstraZeneca, Covis Pharma, Sanofi, Teva, and Thorasys Inc.; and an honorarium as an invited speaker from Covis Pharma, Jean-Coutu Pharmacy, and Brunet Pharmacy. All other authors have no conflict of interest.
Figures
References
-
- Rong G, Zheng Y, Chen Y, Zhang Y, Zhu P, Sawan M. 2023. COVID-19 diagnostic methods and detection techniques. Encyclopedia of Sensors and Biosensors:17–32. doi: 10.1016/B978-0-12-822548-6.00080-7 - DOI
-
- Smith-Jeffcoat SE, Mellis AM, Grijalva CG, Talbot HK, Schmitz J, Lutrick K, Ellingson KD, Stockwell MS, McLaren SH, Nguyen HQ, Rao S, Asturias EJ, Davis-Gardner ME, Suthar MS, Kirking HL, Rolfes MA, Biddle JE, Zhu Y, Ledezma K, Pryor K, Sano E, Petrie JG, RVTN-Sentinel Study Group, RVTN-Sentinel Study Group . 2022. SARS-CoV-2 viral shedding and rapid antigen test performance — respiratory virus transmission network, November 2022–May 2023. MMWR Morb Mortal Wkly Rep 73:365–371. doi: 10.15585/mmwr.mm7316a2 - DOI - PMC - PubMed
-
- Beck EJ, Hsieh Y-H, Fernandez RE, Dashler G, Egbert ER, Truelove SA, Garliss C, Wang R, Bloch EM, Shrestha R, Blankson J, Cox AL, Manabe YC, Kickler T, Rothman RE, Redd AD, Tobian AA, Milstone AM, Quinn TC, Laeyendecker O. 2021. Differentiation of SARS-CoV-2 naturally infected and vaccinated individuals in an inner-city emergency department. medRxiv:2021.10.13.21264968. doi: 10.1101/2021.10.13.21264968 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
