

Performance of volume and diameter thresholds in malignancy prediction of solid nodules in lung cancer screening
- PMID: 40456600
- PMCID: PMC12421124
- DOI: 10.1136/thorax-2024-222086
Performance of volume and diameter thresholds in malignancy prediction of solid nodules in lung cancer screening
Abstract
Background: Prospective validation and comparison of the performance of nodule management protocols is limited. The aim of this study was to examine the performance of size and risk thresholds for assessing malignancy in solid nodules at baseline low-dose CT (LDCT) in a lung cancer screening (LCS) programme.
Methods: This was an observational study using data from the SUMMIT Study, a prospective longitudinal study investigating LDCT for LCS. Participants were 55-77 years old and met either the United States Preventative Services Task Force (2013) criteria or had a PLCOm2012 risk of ≥1.3%. LDCTs were reported using computer-aided detection software (Veolity, MeVIS) with semiautomated volumetry. Cancer outcomes were reported for solid nodules reported at baseline CT, with participants represented by the single largest solid nodule where more than one was present. Malignancy risk was stratified by long-axis diameter and volume using predefined size thresholds taken from British Thoracic Society and European Position statement guidelines: a 5/6 mm long axis diameter or 80/100 mm3 volume 'rule out' thresholds for low-risk nodules and ≥300 mm3 or ≥8 mm diameter with or without Brock score ≥10% 'Rule in' thresholds for high-risk nodules.Pearson's χ2 test was used to calculate statistical significance for nominal variables, McNemar's test for comparison of sensitivity/specificity and DeLong' test for comparison of areas under the receiver operating characteristic curve (AUROC). Optimal thresholds were determined with Youden's J statistic. Net benefit calculations were undertaken to compare the existing thresholds with 95% CIs calculated by bootstrap sampling.
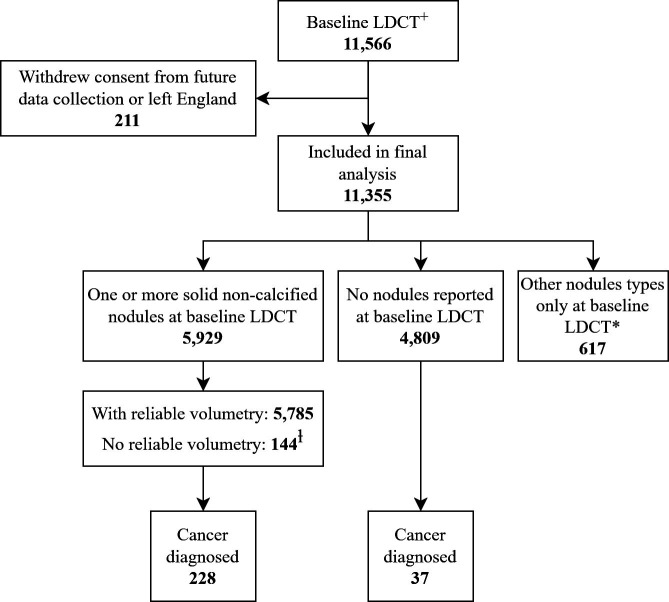
Results: 11 355 participants were included. Crude risk of malignancy in solid nodules at baseline LDCT was 3.8% (228/5929). Risk of malignancy in solid nodules <6 mm long-axis diameter or <100 mm3 volume was equivalent to that in participants with no nodules at baseline LDCT (0.88% and 0.84% vs 0.77%, p=0.4600 and p=0.7932, respectively). A <80 mm3 volume and <5 mm diameter 'rule out' threshold achieved sensitivity 86.8% and 93.4%, specificity 65.4% and 24.64%, and negative predictive value (NPV) 99.2% and 98.9%, respectively. The <80 mm3 volume threshold encompassed 63.3% of participants with a baseline solid nodule compared with 24.0% by the <5 mm diameter threshold.For nodules ≥8 mm diameter, the addition of a risk score (Brock ≥10%) was associated with a significant net benefit when compared with using size threshold alone by net effect analysis (31.24; 95% CI 26.19 to 35.89).
Conclusions: Solid nodules <100 mm3 or <6 mm diameter are not associated with increased risk of lung cancer compared with participants with no nodules at baseline LDCT. Volumetric rule-out thresholds achieve equivalent NPV to long-axis diameter thresholds while encompassing significantly more participants, reducing the number of interval scans required.
Keywords: Imaging/CT MRI etc; Lung Cancer.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: AWC, CH, JLD, ST, HH, PV, RP, AB and CRK are all funded or part-funded through GRAIL as part of the SUMMIT Study. SUMMIT is sponsored and conducted by University College London and funded by GRAIL LLC through a research grant awarded to SMJ as principal investigator. SMJ’s full disclosures are as a Paid Advisory Board member Astra-Zeneca, Bard1 Bioscience, Achilles Therapeutics, Jansen. Assistance for travel to meetings from Astra Zeneca, Takeda, and grant income from GRAIL Inc, Owlstone and share options from Optellum; BARD1 Lifescience. NN is supported by a Medical Research Council Clinical Academic Research Partnership (MR/T02481X/1). NN reports honoraria for non-promotional educational talks or advisory boards from Amgen, Astra Zeneca, Boehringer Ingelheim, Bristol Myers Squibb, EQRx, Fujifilm, Guardant Health, Intuitive, Janssen, Lilly, Merck Sharp & Dohme, Olympus and Roche. AN is part-funded through the UCLH Biomedical Research Centre. AD’s disclosures are personal fees from Boehringer Ingelheim, Roche, Galacto Biotech, Galapagos, Brainomix and Vicore. AH’s disclosures are consulting fees to Evidera and assistance for travel to meetings from GRAIL.
Figures


References
-
- Radiology AC of Lung CT Screening Reporting & Data System (Lung-RADS) 2019
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous