

High diversity of dietary flavonoid intake is associated with a lower risk of all-cause mortality and major chronic diseases
- PMID: 40456886
- PMCID: PMC12283405
- DOI: 10.1038/s43016-025-01176-1
High diversity of dietary flavonoid intake is associated with a lower risk of all-cause mortality and major chronic diseases
Abstract
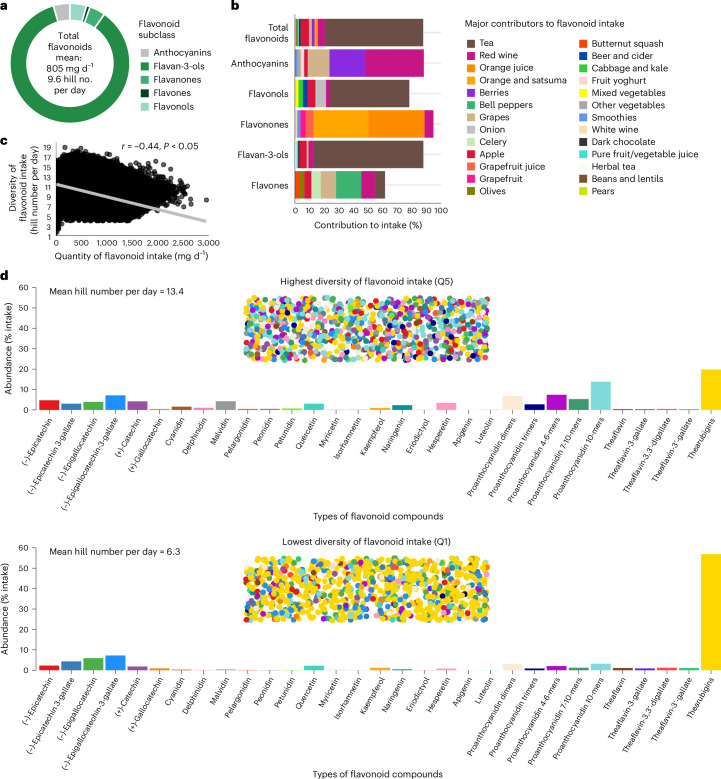
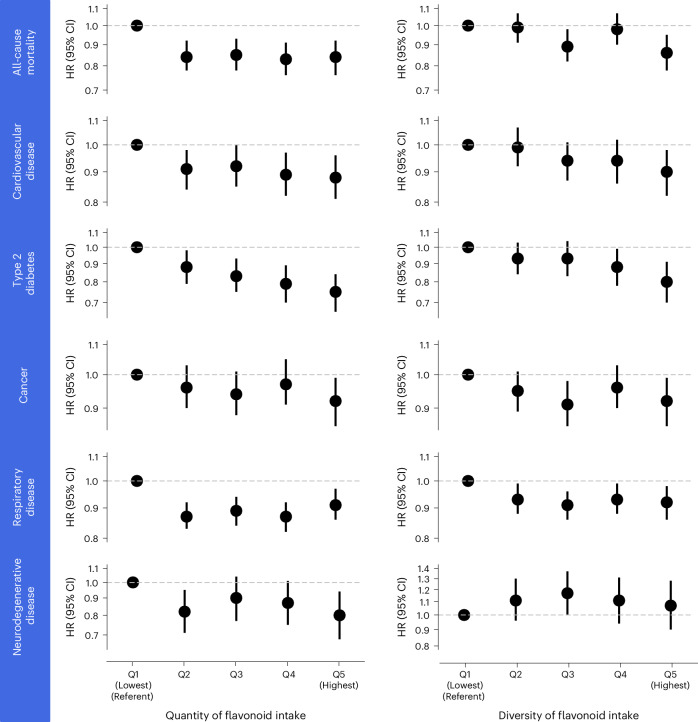
Higher habitual intakes of dietary flavonoids have been linked with a lower risk of all-cause mortality and major chronic disease. Yet, the contribution of diversity of flavonoid intake to health outcomes remains to be investigated. Here, using a cohort of 124,805 UK Biobank participants, we show that participants who consumed the widest diversity of dietary flavonoids, flavonoid-rich foods and/or specific flavonoid subclasses had a 6-20% significantly lower risk of all-cause mortality and incidence of cardiovascular disease, type 2 diabetes, cancer, respiratory disease and neurodegenerative disease. Furthermore, we report that both quantity and diversity of flavonoids are independent predictors of mortality and several chronic diseases, suggesting that consuming a higher quantity and wider diversity is better for longer-term health than either component alone. These findings suggest that consuming several different daily servings of flavonoid-rich foods or beverages, such as tea, berries, apples, oranges or grapes, may lower risk of all-cause mortality and chronic disease.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.C. acts as an advisor to the US Highbush Blueberry Grant Committee (USHBC) and she has received research funding from the USHBC. B.H.P. consults for MaxBiocare, a company engaged in micronutrient research and related commercial activities. The other authors declare no competing interests.
Figures
References
-
- Parmenter, B. H. et al. An overview and update on the epidemiology of flavonoid intake and cardiovascular disease risk. Food Funct.11, 6777–6806 (2020). - PubMed
-
- Hertog, M. G. L. et al. Dietary antioxidant flavonoids and risk of coronary heart disease: the Zutphen Elderly Study. Lancet342, 1007–1011 (1993). - PubMed
-
- Grosso, G. et al. Dietary flavonoid and lignan intake and mortality in prospective cohort studies: systematic review and dose–response meta-analysis. Am. J. Epidemiol.185, 1304–1316 (2017). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
