

Critically ill patients with necrotizing soft tissue infections in the Caribbean area: unsupervised analysis of a retrospective cohort (2014-2023) with identification of factors associated with mortality
- PMID: 40457145
- PMCID: PMC12130383
- DOI: 10.1186/s13613-025-01488-2
Critically ill patients with necrotizing soft tissue infections in the Caribbean area: unsupervised analysis of a retrospective cohort (2014-2023) with identification of factors associated with mortality
Abstract
Background: Scarce epidemiological data are available regarding necrotizing soft tissue infections (NSTIs) in tropical areas. Here we aimed to describe the clinical and biological features, and outcomes, of critically ill patients with NSTIs admitted to an intensive care unit (ICU) in a tropical setting. Furthermore, we analyzed these findings to identify distinct clinical phenotypes and explore their associations with patient outcomes.
Methods: This retrospective observational study included all patients with NSTIs admitted to the ICU of the University Hospital of Guadeloupe between January 2014 and December 2023. Subgroups of patients having similar clinical profiles were identified through unsupervised clustering (factor analysis for mixed data, and hierarchical clustering on principal components). Univariate and multivariate analyses identified factors associated with 90-day mortality.
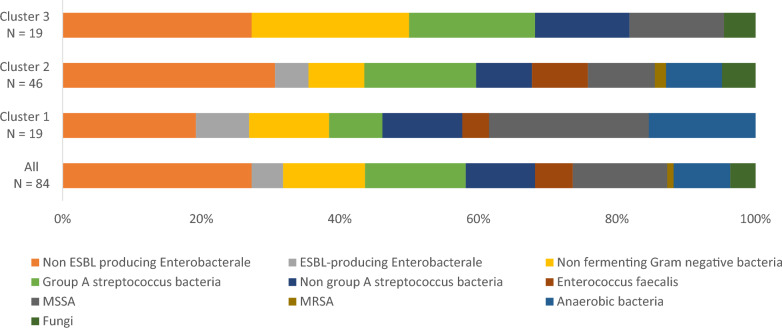
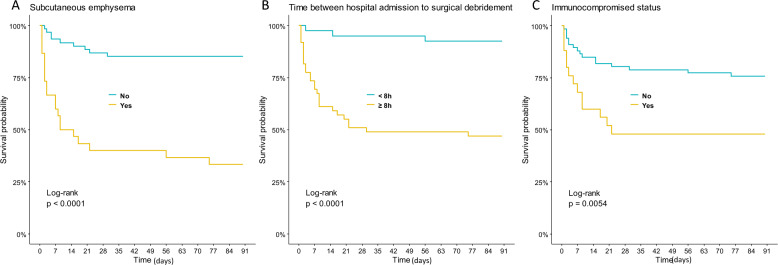
Results: During the study period, 91 NSTI patients were admitted to the ICU. The median Simplified Acute Physiology Score (SAPS) II was 45 [IQR 40-66], and the median time between hospital admission and first surgical debridement was 8 h [IQR 6-10 h]. While in the ICU, 65% of patients were mechanically ventilated, 75% experienced shock, and 34% underwent renal replacement therapy. The 90-day mortality rate was 32%. Unsupervised clustering revealed three clusters-mild NSTI (n = 23, 25%), severe NSTI (n = 49, 54%), and fulminant NSTI (n = 19, 21%)-which were associated with different ICU courses and outcomes. Subcutaneous emphysema and sepsis-associated encephalopathy were key components influencing cluster identification. Multivariate analysis revealed that mortality was associated with SAPS II, subcutaneous emphysema, >8 h between hospital admission and first surgery, and immunocompromised status.
Conclusion: Unsupervised analysis of critically ill patients with NSTIs in tropical settings revealed three distinct patient clusters that exhibited unique phenotypic characteristics and clinical outcomes. Upon hospital admission, patients with NSTIs should be carefully screened for sepsis-associated encephalopathy, subcutaneous emphysema, and thrombopenia. The present exploratory results must be confirmed in larger multicentric cohorts.
Keywords: Fasciitis; Intensive care unit; Multiple-organ failure; Necrotizing soft tissue infection; Septic shock.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was performed in accordance with the declaration of Helsinki for research including human data. The study was approved by the local ethics committee, which waived consent for retrospective anonymous data collection, in accordance with French Law, and was registered under the number A26_20/02/2024. This study is reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. All authors have given consent for publication of this manuscript in Annals of Intensive Care. Competing interests: The authors declare that they have no competing interests.
Figures
Similar articles
-
Healthcare trajectory of critically ill patients with necrotizing soft tissue infections: a multicenter retrospective cohort study using the clinical data warehouse of Greater Paris University Hospitals.Ann Intensive Care. 2022 Dec 20;12(1):115. doi: 10.1186/s13613-022-01087-5. Ann Intensive Care. 2022. PMID: 36538244 Free PMC article.
-
Organ Involvement Related to Death in Critically Ill Patients With Leptospirosis: Unsupervised Analysis in a French West Indies ICU.Crit Care Explor. 2024 Jul 8;6(7):e1126. doi: 10.1097/CCE.0000000000001126. eCollection 2024 Jul 1. Crit Care Explor. 2024. PMID: 38980049 Free PMC article.
-
Necrotizing Soft Tissue Infections in Intensive Care.J Intensive Care Med. 2022 Mar;37(3):393-400. doi: 10.1177/08850666211010127. Epub 2021 Apr 26. J Intensive Care Med. 2022. PMID: 33896254 Free PMC article.
-
Using clinical pathways to aid in the diagnosis of necrotizing soft tissue infections synthesis of evidence.Worldviews Evid Based Nurs. 2012 Apr;9(2):88-99. doi: 10.1111/j.1741-6787.2011.00235.x. Epub 2011 Dec 12. Worldviews Evid Based Nurs. 2012. PMID: 22151905 Review.
-
Time is of the essence when treating necrotizing soft tissue infections: a systematic review and meta-analysis.World J Emerg Surg. 2020 Jan 8;15:4. doi: 10.1186/s13017-019-0286-6. eCollection 2020. World J Emerg Surg. 2020. PMID: 31921330 Free PMC article.
References
-
- Peetermans M, De Prost N, Eckmann C, Norrby-Teglund A, Skrede S, De Waele JJ. Necrotizing skin and soft-tissue infections in the intensive care unit. Clin Microbiol Infect. 2020;26(1):8–17. - PubMed
-
- Hua C, Urbina T, Bosc R, et al. Necrotising soft-tissue infections. Lancet Infect Dis. 2023;23(3):e81–94. - PubMed
-
- Boyer A, Vargas F, Coste F, et al. Influence of surgical treatment timing on mortality from necrotizing soft tissue infections requiring intensive care management. Intensive Care Med. 2009;35(5):847–53. - PubMed
LinkOut - more resources
Full Text Sources
