

Estimating the societal costs and benefits of de-implementation of low-value care: developing a modelling approach through case assessment
- PMID: 40457258
- PMCID: PMC12128256
- DOI: 10.1186/s12913-025-12948-7
Estimating the societal costs and benefits of de-implementation of low-value care: developing a modelling approach through case assessment
Abstract
Background: Previous estimates of potential costs savings from de-implementation of low-value care have been calculated with simple modelling approaches, focused on direct medical costs and did not take substitution into account. Therefore, the aim of this study was to develop and evaluate a modelling approach to calculate a more realistic estimate of societal costs and benefits of de-implementation of low-value care.
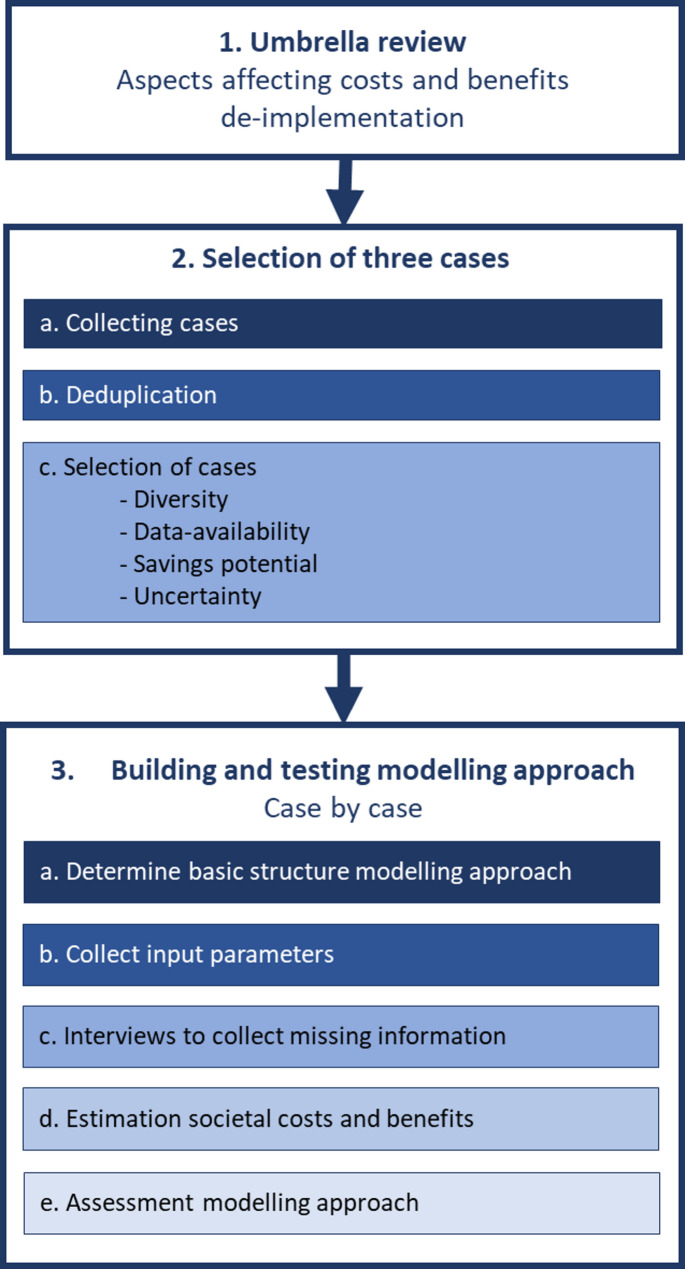
Methods: The modelling approach was developed and evaluated in three steps: (1) review of reviews to identify aspects that may affect the costs and benefits of de-implementation, (2) selection of three cases of low-value care, (3) development and evaluation of the modelling approach for each case. Desk research and interviews with actors were used in step 3 to define input parameters.
Results: The modelling approach was build and evaluated for the following cases: (1) surgery for achilles tendon rupture, (2) mammography for women < 30 years with focal breast complaints, and (3) imaging for non-specific low back pain. From the interviews, it appeared that case 2 had already been fully disinvested. Hence, calculating the societal costs and benefits for this case was not considered valuable. For case 1 and 3 it was considered valuable and feasible to calculate the societal costs and benefits. Compared to the adapted societal business case approach used in case 1, the adapted societal cost-benefit analysis approach used for case 3 provided a more realistic and better estimate.
Conclusions: It is feasible to calculate a more elaborate and realistic estimate of societal costs and benefits of the de-implementation of low-value care than previous estimates. Nevertheless, it was not feasible to include the costs of de-implementation itself as these are highly reliant on the specific de-implementation strategy employed, which is context specific. Furthermore, the time needed to calculate a more elaborate and realistic estimate stresses the need to carefully select low-value care cases for which the value of calculating such an elaborate and realistic estimate outweighs the effort required to do so.
Supplementary Information: The online version contains supplementary material available at 10.1186/s12913-025-12948-7.
Keywords: Cost savings; De-implementation; Low-value care; Modelling approach; Societal costs and benefits.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The research project has been assessed by the Centre for Clinical Expertise (CCE) at the National Institute for Public Health and the Environment (RIVM) in the Netherlands (study number: VPZ-605). The CCE concluded that the research project is exempted from further review by a medical ethics committee as it does not fulfil the specific conditions as stated in the Dutch Medical Research Involving Human Subjects Act. At the start of the interviews, participants were asked oral informed consent for participation in this study. The authors complied with the European ALLEA code of conduct for research integrity and the Dutch code of conduct on scientific integrity. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Estimating the Societal Benefits of THA After Accounting for Work Status and Productivity: A Markov Model Approach.Clin Orthop Relat Res. 2016 Dec;474(12):2645-2654. doi: 10.1007/s11999-016-5084-9. Epub 2016 Oct 3. Clin Orthop Relat Res. 2016. PMID: 27699631 Free PMC article.
-
Surgery for hip fracture yields societal benefits that exceed the direct medical costs.Clin Orthop Relat Res. 2014 Nov;472(11):3536-46. doi: 10.1007/s11999-014-3820-6. Epub 2014 Aug 5. Clin Orthop Relat Res. 2014. PMID: 25091223 Free PMC article.
-
A societal cost-benefit analysis of falls prevention in community-dwelling older people in the Netherlands.Exp Gerontol. 2025 Jun 15;205:112755. doi: 10.1016/j.exger.2025.112755. Epub 2025 Apr 17. Exp Gerontol. 2025. PMID: 40252716
-
Cost Controversies of a "Home Dialysis First" Policy.Can J Kidney Health Dis. 2019 Aug 30;6:2054358119871541. doi: 10.1177/2054358119871541. eCollection 2019. Can J Kidney Health Dis. 2019. PMID: 31516718 Free PMC article. Review.
-
The Economic Impact of Smoking and of Reducing Smoking Prevalence: Review of Evidence.Tob Use Insights. 2015 Jul 14;8:1-35. doi: 10.4137/TUI.S15628. eCollection 2015. Tob Use Insights. 2015. PMID: 26242225 Free PMC article. Review.
References
-
- Vonk R, Hilderink H, Plasmans M, Kommer G, Polder J. Health care expenditures foresight 2015–2060: quantitative preliminary study at the request of the scientific Council for government policy (WRR). Part 1: future projections. Bilthoven: Rijksinstituut voor Volksgezondheid en Milieu; 2020.
-
- Zorginstituut Nederland. Totale zorgkosten Zorgverzekeringswet Diemen: Zorginstituut Nederland; 2024.Available from: https://www.zorgcijfersdatabank.nl/. Accessed 4 June 2024.
-
- Organisation for Economic Co-operation and Development. Health expenditure and financing. 2024. Available from: https://stats.oecd.org/WBOS/index.aspx. Accessed 4 June 2024.
-
- van der Woude D, Heida JP, van der Erf S. Geschat potentieel effectieve Zorg: Schatting opbrengst focus op effectieve Zorg in basispakket. Strategies in Regulated Markets; 2021.
-
- ActiZ, De Nederlandse ggz et al. Federatie Medisch Specialisten, InEen, Nederlandse Federatie van Universitair Medische Centra, Nederlandse Vereniging van Ziekenhuizen,. Integraal Zorg Akkoord: Samen werken aan gezonde zorg. Ministerie van Volksgezondheid, Welzijn en Sport; 2022.
Grants and funding
LinkOut - more resources
Full Text Sources
