

Effect of ERAS pathway nursing on postoperative rehabilitation of patients undergoing gastrointestinal surgery: a meta-analysis
- PMID: 40457265
- PMCID: PMC12128559
- DOI: 10.1186/s12893-025-02976-9
Effect of ERAS pathway nursing on postoperative rehabilitation of patients undergoing gastrointestinal surgery: a meta-analysis
Abstract
Background: This study aimed to systematically evaluate the impact of the Enhanced Recovery After Surgery (ERAS) pathway on postoperative outcomes-including hospital length of stay, complication rates, readmission, reoperation, and mortality-in patients undergoing gastrointestinal surgery, to provide evidence-based guidance for clinical practice.
Methods: We systematically searched PubMed, Cochrane Library, Embase, Web of Science and Scopus databases for randomized controlled trials (RCTs) and cohort studies on ERAS pathway in postoperative rehabilitation. Thirteen studies comprising a total of 5,603 patients were included. Literature screening and quality assessment followed the standards of Cochrane Collaboration and Newcastle-Ottawa scales. Statistical analysis was performed using R software to calculate the relative risk (RR), mean difference (MD) with 95% confidence interval (CI), and heterogeneity through the I² statistic, with significance set at P < 0.05. This systematic review and meta-analysis has been registered in the PROSPERO database (ID: CRD42024608876).
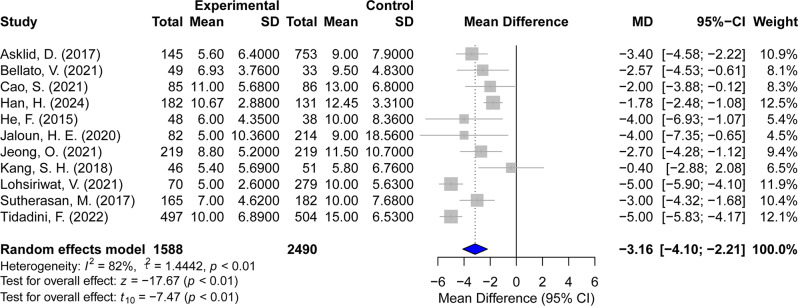
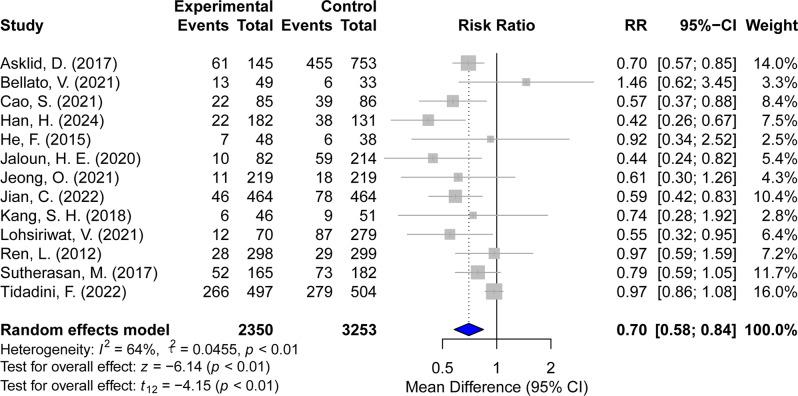
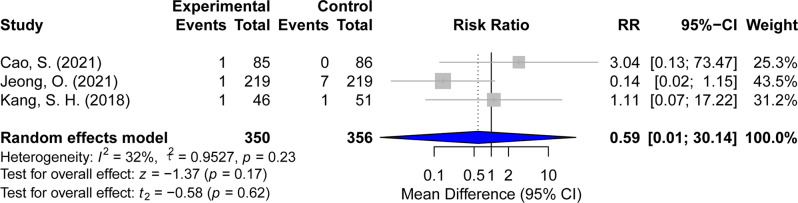
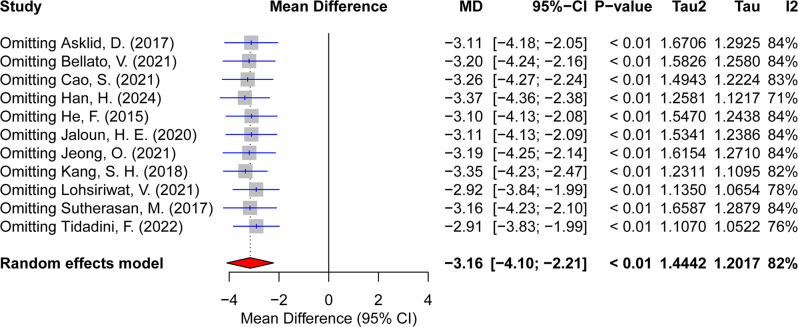
Results: The ERAS pathway significantly shortened the postoperative hospital stay (MD = -3.16, 95% CI [-4.10, -2.21], P < 0.01) and reduced the incidence of postoperative complications (RR = 0.70, 95% CI [0.58, 0.84], P < 0.01). It also significantly reduced the readmission rates (RR = 0.75, 95% CI [0.58, 0.96], P = 0.02). However, there was no statistically significant difference in the impact of ERAS pathway on reoperation rate and mortality (RR = 0.59, 95% CI [0.01, 30.14], P = 0.62).
Conclusions: ERAS protocols are associated with improved postoperative recovery in gastrointestinal surgery, including shorter hospital stays and reduced complication and readmission rates. Although no significant effects were found for reoperation or mortality, the overall evidence supports the broader clinical adoption of ERAS, with a need for further high-quality studies to address remaining uncertainties.
Keywords: Enhanced recovery after surgery; Gastrointestinal surgical procedures; Meta-analysis; Postoperative care; Postoperative complications; Systematic review.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent of participate: As this study is a systematic review and meta-analysis of previously published studies, ethical approval and informed consent were not required. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Perioperative enhanced recovery programmes for women with gynaecological cancers.Cochrane Database Syst Rev. 2022 Mar 15;3(3):CD008239. doi: 10.1002/14651858.CD008239.pub5. Cochrane Database Syst Rev. 2022. PMID: 35289396 Free PMC article.
-
Fast track surgery versus conventional recovery strategies for colorectal surgery.Cochrane Database Syst Rev. 2011 Feb 16;(2):CD007635. doi: 10.1002/14651858.CD007635.pub2. Cochrane Database Syst Rev. 2011. PMID: 21328298
-
Limited versus full sternotomy for aortic valve replacement.Cochrane Database Syst Rev. 2017 Apr 10;4(4):CD011793. doi: 10.1002/14651858.CD011793.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2023 Dec 6;12:CD011793. doi: 10.1002/14651858.CD011793.pub3. PMID: 28394022 Free PMC article. Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Prosthetic mesh placement for the prevention of parastomal herniation.Cochrane Database Syst Rev. 2018 Jul 20;7(7):CD008905. doi: 10.1002/14651858.CD008905.pub3. Cochrane Database Syst Rev. 2018. PMID: 30027652 Free PMC article.
References
-
- Engelman DT, Ben Ali W, Williams JB, Perrault LP, Reddy VS, Arora RC, Roselli EE, Khoynezhad A, Gerdisch M, Levy JH, et al. Guidelines for perioperative care in cardiac surgery: enhanced recovery after surgery society recommendations. JAMA Surg. 2019;154(8):755–66. - PubMed
-
- Nelson G, Fotopoulou C, Taylor J, Glaser G, Bakkum-Gamez J, Meyer LA, Stone R, Mena G, Elias KM, Altman AD, et al. Enhanced recovery after surgery (ERAS®) society guidelines for gynecologic oncology: addressing implementation challenges– 2023 update. Gynecol Oncol. 2023;173:58–67. - PubMed
-
- Zaouter C, Imbault J, Labrousse L, Abdelmoumen Y, Coiffic A, Colonna G, Jansens JL, Ouattara A. Association of robotic totally endoscopic coronary artery bypass graft surgery associated with a preliminary cardiac enhanced recovery after surgery program: A retrospective analysis. J Cardiothorac Vasc Anesth. 2015;29(6):1489–97. - PubMed
-
- Stenberg E, Dos Reis Falcão LF, O’Kane M, Liem R, Pournaras DJ, Salminen P, Urman RD, Wadhwa A, Gustafsson UO, Thorell A. Guidelines for perioperative care in bariatric surgery: enhanced recovery after surgery (ERAS) society recommendations: A 2021 update. World J Surg. 2022;46(4):729–51. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
