

Prioritizing circulation over airway to improve survival in trauma patients with exsanguinating injuries: a world society of emergency surgery-panamerican trauma consensus statement
- PMID: 40457450
- PMCID: PMC12128548
- DOI: 10.1186/s13017-025-00618-2
Prioritizing circulation over airway to improve survival in trauma patients with exsanguinating injuries: a world society of emergency surgery-panamerican trauma consensus statement
Abstract
Introduction: Hemorrhage is one of the leading causes of preventable death in trauma patients. For decades, the Airway-Breathing-Circulation (ABC) approach has been the cornerstone of trauma care. However, emerging evidence suggests that prioritizing airway management in exsanguinating patients may worsen hypotension and increase mortality. This systematic review and meta-analysis aim to evaluate the effectiveness of the Circulation-Airway-Breathing (CAB) approach compared to the traditional ABC sequence in improving survival in trauma patients with severe hemorrhage.
Methods: A systematic review was conducted in accordance with the PRISMA guidelines. Databases including PubMed and Ovid MEDLINE, SCOPUS, web of science and EMBASE were searched for studies published up to September 2024. Eligible studies included observational and comparative studies reporting outcomes of trauma patients with exsanguinating hemorrhage. The Newcastle-Ottawa Scale was used for risk of bias assessment. A meta-analysis was performed using a random-effects model to calculate pooled odds ratios (OR) for mortality, with 95% confidence intervals (CI). Subgroup analysis was conducted to compare the ABC and CAB approaches in prospective and retrospective studies.
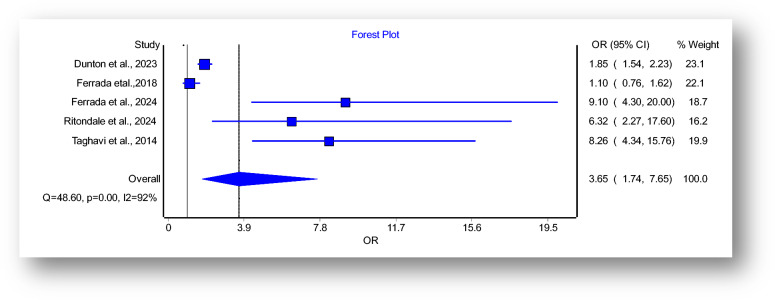
Results: Six studies (N = 11,855 patients) met the inclusion criteria. The meta-analysis revealed a significant increase in mortality associated with the ABC approach (pooled OR: 3.65, 95% CI: 1.74-7.65). Subgroup analysis of prospective cohort studies found an even higher mortality risk (POR: 9.99, 95% CI: 5.59-17.85) when compared with POR of retrospective studies (POR: 2.42, 95%CI: 1.08-5.36). High heterogeneity (I2 = 92%) was observed across the studies, likely due to variations in patient populations and resuscitation protocols.
Conclusion: Prioritizing circulation over airway management in trauma patients with exsanguinating injuries significantly reduces mortality compared to the traditional ABC approach. The present consensus paper, conducted according to the WSES methodology3, aims to provide a review of the literature comparing the CAB approach to the traditional ABC sequence in trauma patients with exsanguinating hemorrhage, to develop a shared consensus statement based on the currently available evidence.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This is a consensus statement and does not require an ethics declaration. “Ethics declaration: Not applicable”. Competing interests: There are no competing interests or conflicts of interest to declare pertinent to this manuscript.
Figures


References
-
- 10th Edition of the Advanced Trauma Life Support ® (ATLS ® ) Student Course Manual. Chicago (IL): American College of Surgeons; 2018.
-
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schünemann HJ. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–6. 10.1136/bmj.39489.470347.AD. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
