

Accuracy of the modified Global Burden of Disease International Classification of Diseases coding methods for identifying sepsis: a prospective multicentre cohort study
- PMID: 40457465
- PMCID: PMC12128331
- DOI: 10.1186/s13054-025-05448-x
Accuracy of the modified Global Burden of Disease International Classification of Diseases coding methods for identifying sepsis: a prospective multicentre cohort study
Abstract
Background: This study assessed the accuracy of three International Classification of Diseases (ICD) codes methods derived from Global Burden of Disease (GBD) sepsis study (modified GBD method) in identifying sepsis, compared to the Angus method. Sources of errors in these methods were also reported.
Methods: Prospective multicentre, observational, study. Emergency Department patients aged ≥ 16 years with high sepsis risk from nine hospitals in NSW, Australia were screened for clinical sepsis using Sepsis 3 criteria and coded as having sepsis or not using the modified GBD and Angus methods. The three modified GBD methods were: Explicit-sepsis-specific ICD code recorded; Implicit-sepsis-specific code or infection as primary ICD code plus organ dysfunction code; Implicit plus-as for Implicit but infection as primary or secondary ICD code. Agreement between clinical sepsis and ICD coding methods was assessed using Cronbach alpha (α). For false positive cases (ICD-coded sepsis but not clinically diagnosed), the ICD codes leading to those errors were documented. For false negatives (clinically diagnosed sepsis but ICD-coded), uncoded sources of infection and organ dysfunction were documented.
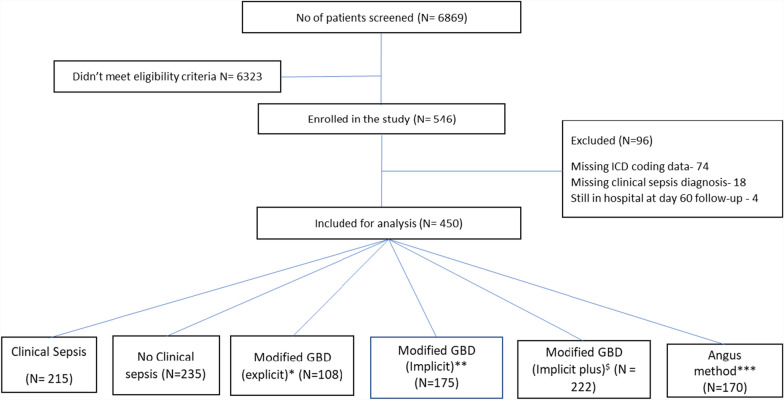
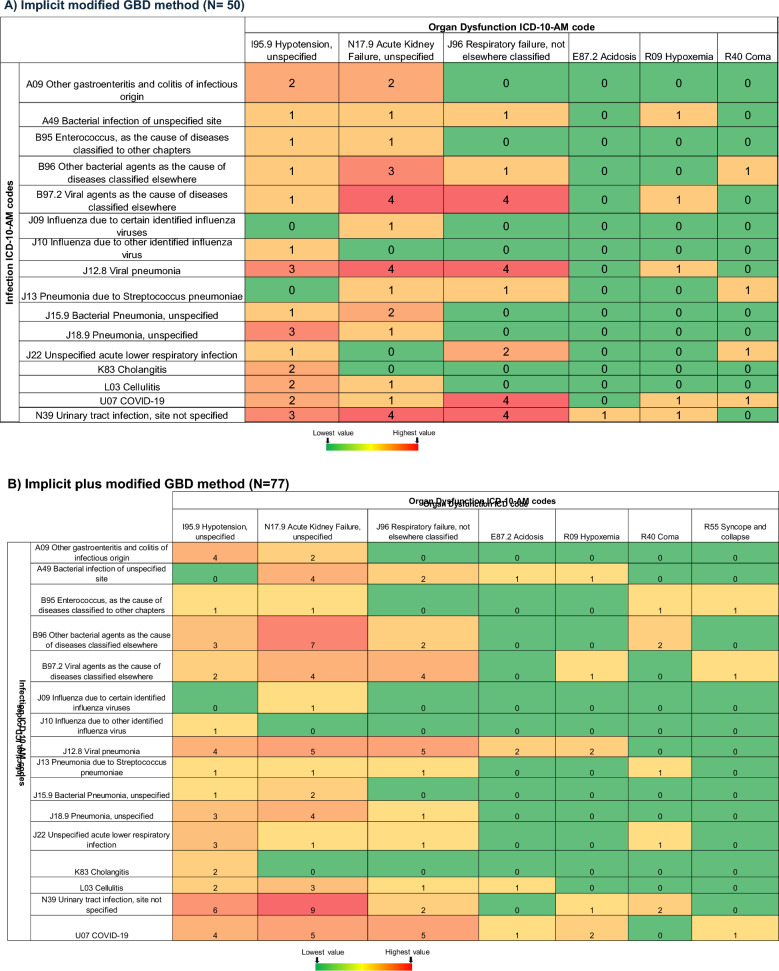
Results: Of 6869 screened patients, 450 (median age 72.4 years, 48.9% females) met inclusion criteria. Clinical sepsis was diagnosed in 215/450 (47.8%). The explicit, implicit, implicit plus and Angus methods identified sepsis in 108/450 (24.0%), 175/450 (38.9%), 222/450 (49.3%) and 170/450 (37.8%), respectively. Sensitivity was 41.4%, 58.1%, 67.4% and 55.8%, and specificity 91.9%, 78.7%, 67.2% and 79.1%, respectively. Agreement between clinical sepsis and all ICD coding methods was low (α = 0.52-0.56). False positives were 19, 50, and 77, while false negatives were 126, 90, and 70 for the explicit, implicit, and implicit plus methods, respectively. For false positive cases, unspecified urinary tract infection, hypotension and acute kidney failure were commonly assigned infection and organ dysfunction codes. About half (44.3%-55.6%) of the false negative cases didn't have a pathogen documented.
Conclusion: The modified GBD method demonstrated low accuracy in identifying sepsis; with the implicit plus method being the most accurate. Errors in identifying sepsis using ICD codes arise mostly from coding for unspecified urinary infections and associated organ dysfunction.
Trial registration: The study was registered at the ANZCTR (ACTRN12621000333819) on 24 March 2021.
Keywords: Diagnostic accuracy; ICD code; Sensitivity; Sepsis; Specificity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and was approved by the Southwestern Sydney Local Health District Human Research Ethics Committee (approval number 2020/ETH00180, dated 14 May 2020). This was a low/negligible risk observational study using demographic, physiological and patient data which is measured routinely as part of clinical care. Moreover, there was no clinical risk associated for participants as the study was observational in nature and has no potential to interfere with standard treatment. There was no risk to the rights, privacy or professional reputation of carers, health professionals and/or institutions as the study solely concerns with analysis of clinical data collected as part of standard clinical care. Hence, ethical approval was obtained with a waiver of individual patient consent in keeping with local guidelines on the conduct of research in humans and complying with state and Federal privacy laws. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
-
- Global Sepsis Agenda 2030. Accessible from: https://globalsepsisalliance.org/20230-global-agenda-for-sepsis
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
