

The value of dynamic cerebral compliance monitoring after pediatric traumatic brain injury: a STARSHIP study sub-analysis
- PMID: 40457466
- PMCID: PMC12128296
- DOI: 10.1186/s13054-025-05403-w
The value of dynamic cerebral compliance monitoring after pediatric traumatic brain injury: a STARSHIP study sub-analysis
Abstract
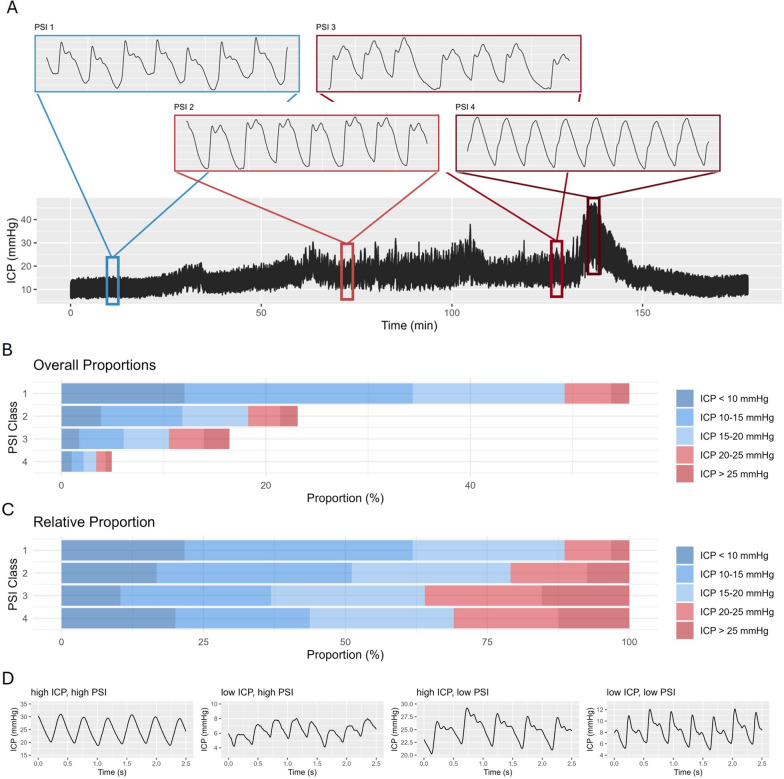
Introduction: Cerebral compliance describes the pressure-volume relationship within the intracranial space, quantifying the brain's capacity to accommodate changes in volume before significant increases in intracranial pressure (ICP) occur. The pulse shape index - PSI-classifies the ICP pulse-wave-configuration into 4 categories representing the incremental state of compliance. In this analysis we explore the metric in a cohort of prospectively collected pediatric TBI patients in relation to outcome, physiological parameters, and individual ICP insults.
Methodology: Data acquired by the prospective observational STARSHIP study which included clinical information, 12-month outcome, and monitoring data from 98 pediatric TBI patients admitted to 10 pediatric intensive care units across the UK was assessed. PSI was calculated and compared using univariable and multivariable analyses, as well as considering their time-trends and relation to individual ICP insults.
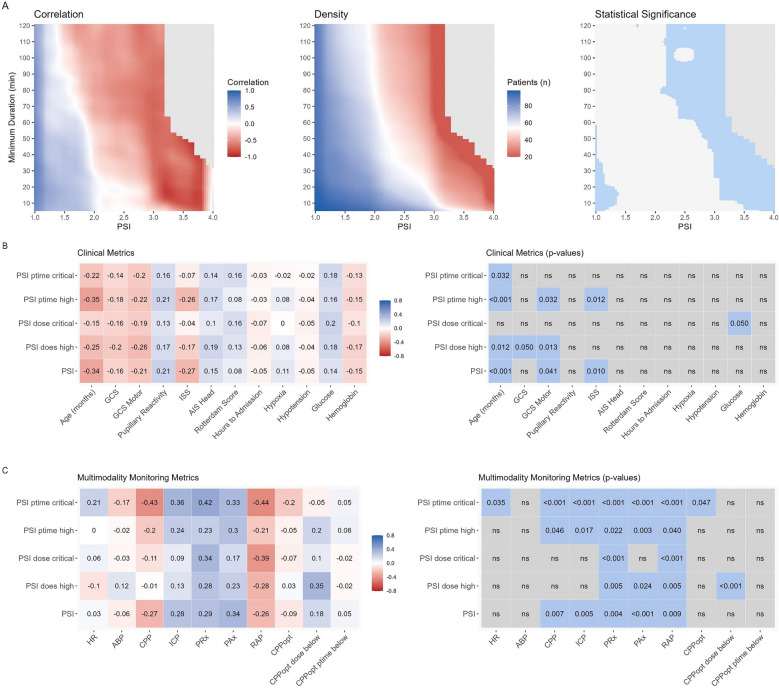
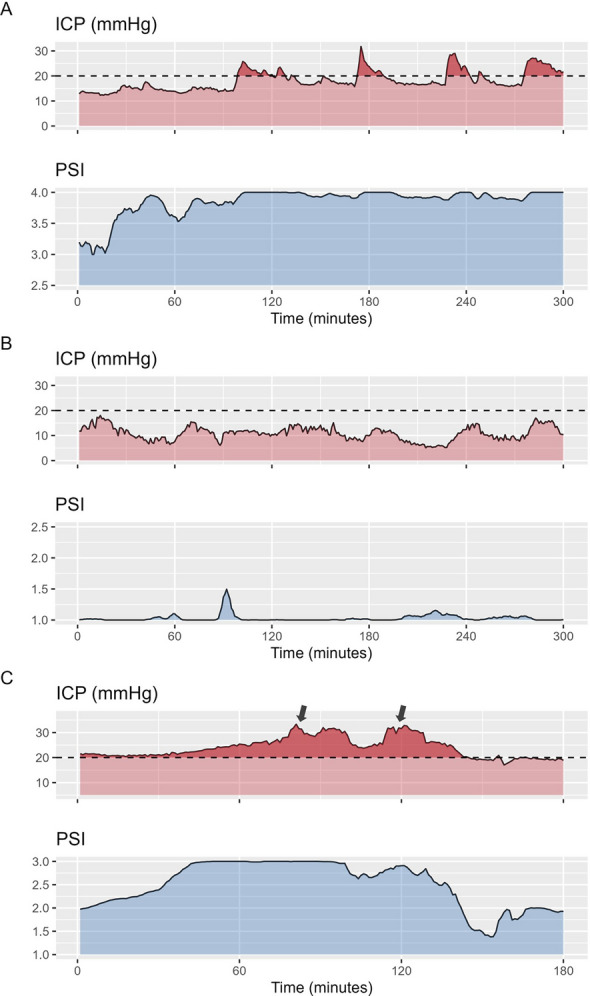
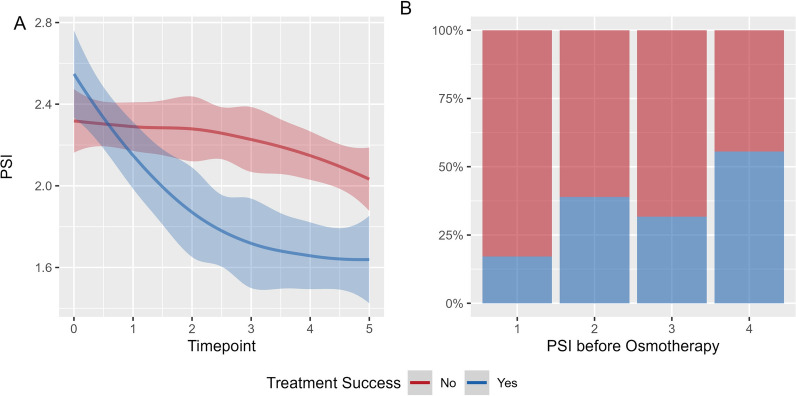
Results: PSI derived metrics were associated with outcomes within univariable analyses, additionally they were associated with ICP, and worse cerebrovascular reactivity (absolute correlation coefficients close to 0.3 for the described metrics). Cross correlation analysis revealed a median delay of 8 min for changes in ICP after changes in PSI (95% confidence interval of 7.6 to 8.5 min). Higher PSI value before ICP elevations was associated with longer duration and greater magnitude of subsequent ICP insults. Additionally, higher PSI before and faster decrease in PSI after osmotherapy were associated with successful reduction of ICP.
Conclusions: PSI enhances bedside monitoring of pediatric TBI by enabling dynamic assessment of cerebral compliance. Variations in PSI appear to precede subsequent ICP insults and are associated with their severity, thereby potentially facilitating timely interventions. Furthermore, assessing the PSI level before administering osmotherapy may allow gauging treatment success.
Keywords: Compliance; Multimodality monitoring; Osmotherapy; Traumatic brain injury; Treatment.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: The STARSHIP trial was approved by the Health Research Authority, Southwest-Central Bristol Research Ethics Committee (Ref: 18/SW/0053). Consent to participate: Due to the observational nature of the acute phase of the project, a deferred consent for acute data collection and sharing was taken to allow for the acquisition of a bias-free sample. Informed consent was received by the patients’ legal guardian for data sharing and follow-up before discharge. Consent to publish: Not applicable. Competing interests: Peter Smielewski and Marek Czosnyka receive part of the licensing fees for ICM + software, licensed by Cambridge Enterprise Ltd, University of Cambridge, Cambridge. The other authors declare no financial or non-financial conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
