

Incarceration of the Afferent Loop into the Sutured Closed Mesenteric Defect after Gastrectomy Followed by Billroth-II Reconstruction for Gastric Cancer: Two Case Reports
- PMID: 40458128
- PMCID: PMC12129561
- DOI: 10.70352/scrj.cr.25-0167
Incarceration of the Afferent Loop into the Sutured Closed Mesenteric Defect after Gastrectomy Followed by Billroth-II Reconstruction for Gastric Cancer: Two Case Reports
Abstract
Introduction: Internal hernia is a critical complication after laparoscopic gastrectomy with Roux-en-Y, Billroth-II or double tract reconstruction. It is recommended that mesenteric defects should be closed to prevent internal hernias. We reported two patients who developed internal hernias, in which the afferent loop of Billroth-II reconstruction became incarcerated into the closed mesenteric defects.
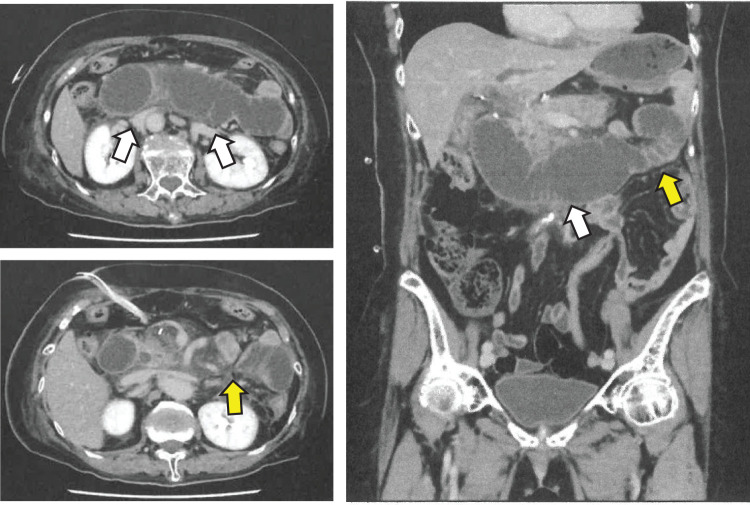
Case presentation: A man in his late 40s had undergone laparoscopic distal gastrectomy 3 months prior for gastric cancer followed by Billroth-II reconstruction, in which mesenteric defect was sutured closed. The patient visited our hospital complaining of sudden severe upper abdominal pain and was diagnosed with afferent loop obstruction due to an incarcerated internal hernia complicated by acute pancreatitis. Emergency surgery, in which intestinal incarceration was relieved and intestinal ischemia was not found, was performed on the same day as admission. However, postoperative duodenal microperforation occurred, making treatment difficult. A woman in her late 70s had undergone laparoscopic distal gastrectomy 7 days prior for gastric cancer followed by Billroth-II reconstruction, in which mesenteric defect was sutured closed. The patient complained of nausea without abdominal pain and was diagnosed with afferent loop obstruction due to an incarcerated internal hernia. Emergency surgery, in which intestinal incarceration was relieved and intestinal ischemia was not found, was performed on the same day. The patient was discharged uneventfully. In both cases, a hernia orifice formed in the Treiz ligament area, and the afferent loop was incarcerated into the closed mesenteric defect.
Conclusions: Incarcerated internal hernias should be treated as soon as possible. Although closure of the mesenteric defects after Billroth-II reconstruction is necessary to prevent internal hernias, mesenteric defects should be closed on the left side as far away from the Treiz ligament as possible.
Keywords: Billroth-II reconstruction; gastric cancer; internal hernia; laparoscopic surgery; mesenteric defect.
© 2025 The Author(s). Published by Japan Surgical Society.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






References
-
- Dikken JL, Lemmens VE, Wouters MW, et al. Increased incidence and survival for oesophageal cancer but not for gastric cardia cancer in the Netherlands. Eur J Cancer 2012; 48: 1624–32. - PubMed
-
- Xie SH, Lagergren J. Time trends in the incidence of oesophageal cancer in Asia: variations across populations and histological types. Cancer Epidemiol 2016; 44: 71–6. - PubMed
-
- Deans C, Yeo MS, Soe MY, et al. Cancer of the gastric cardia is rising in incidence in an Asian population and is associated with adverse outcome. World J Surg 2011; 35: 617–24. - PubMed
-
- Matsuno K, Ishihara R, Ohmori M, et al. Time trends in the incidence of esophageal adenocarcinoma, gastric adenocarcinoma, and superficial esophagogastric junction adenocarcinoma. J Gastroenterol 2019; 54: 784–91. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials