

Association between triglyceride-glucose index and the risk of cardiometabolic diseases in metabolically healthy obese individuals: a prospective cohort study
- PMID: 40458180
- PMCID: PMC12127177
- DOI: 10.3389/fendo.2025.1524786
Association between triglyceride-glucose index and the risk of cardiometabolic diseases in metabolically healthy obese individuals: a prospective cohort study
Abstract
Background: Metabolically healthy obese (MHO) individuals meet the criteria for obesity with normal blood glucose and lipid metabolism parameters, absence of hypertension, and no concurrent cardiovascular diseases. However, the association between the triglyceride-glucose (TyG) index and the risk of cardiometabolic disease (CMD) in MHO individuals remains unclear.
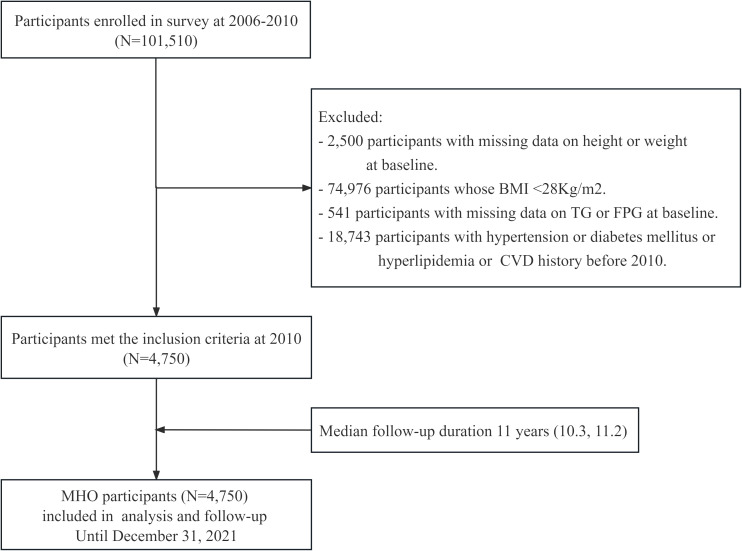
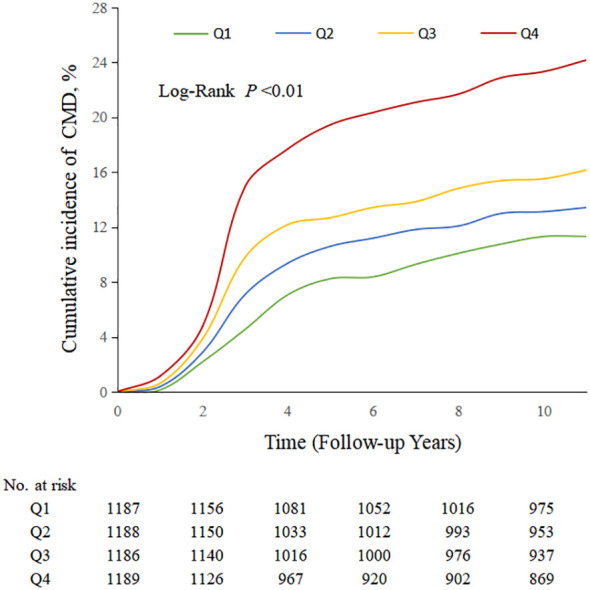
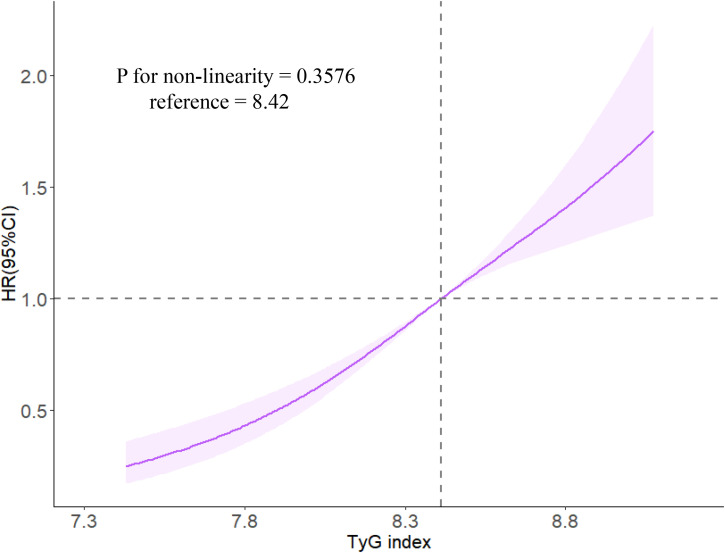
Methods and results: This study included obese individuals who underwent health examinations at Kailuan Group from 2006 to 2010, whom without a history of hypertension, diabetes, hyperlipidemia, cardiovascular disease, as the study participants. A total of 4750 participants were included in this study. The TyG index was calculated as ln[TG (mg/dL) × FPG (mg/dL)/2] and divided into four groups based on quartiles: Q1 group (<8.18); Q2 group (8.18-8.41); Q3 group (8.42-8.62); Q4 group (≥8.63). The Cox proportional hazards model was used to assess the relationship between the TyG index and risk of CMD incidence. During a median follow-up period of 11 (IQR 10.3, 11.2) years, 826 participants experienced CMD, among whom 131 participants developed coronary heart disease, 215 participants developed stroke, and 542 participants developed diabetes. After adjusting for multiple confounding factors, compared with the Q1 group, the adjusted HRs (95% CI) for CMD in the Q2-Q4 groups were 1.33 (1.03, 1.65), 1.37 (1.04, 1.82), and 2.04 (1.56, 2.68) (P<0.0001). A similar trend was found in the subtypes of CMD in coronary heart disease, stroke, and diabetes. Restrictive cubic spline analysis revealed a linear dose-response relationship between the TyG index and the risk of CMD.
Conclusions: A high TyG index increases the risk of CMD in MHO individuals. Monitoring and maintaining an appropriate TyG index may contribute to the prevention of CMD risk in MHO individuals.
Keywords: cardiometabolic disease; coronary heart disease; diabetes; metabolically healthy obese; stroke; triglyceride-glucose index.
Copyright © 2025 Chen, Wu, Cai, Wu, Zheng, Fu, Wang, Wang, Lan, Chen, Wu and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Figures
Similar articles
-
Change in triglyceride-glucose index predicts the risk of cardiovascular disease in the general population: a prospective cohort study.Cardiovasc Diabetol. 2021 May 26;20(1):113. doi: 10.1186/s12933-021-01305-7. Cardiovasc Diabetol. 2021. PMID: 34039351 Free PMC article.
-
Impact of triglyceride-glucose index on risk of cardiovascular disease among non-diabetic hypertension patients: a 10-year prospective cohort study.BMC Public Health. 2025 Jan 25;25(1):326. doi: 10.1186/s12889-025-21522-z. BMC Public Health. 2025. PMID: 39863839 Free PMC article.
-
Triglyceride-glucose index associated with the risk of cardiovascular disease: the Kailuan study.Endocrine. 2022 Feb;75(2):392-399. doi: 10.1007/s12020-021-02862-3. Epub 2021 Sep 20. Endocrine. 2022. PMID: 34542800
-
Impact of the Triglyceride-Glucose index on all-cause and cardiovascular mortalities across different metabolic health and obesity statuses in US adults.BMC Public Health. 2025 May 14;25(1):1767. doi: 10.1186/s12889-025-22901-2. BMC Public Health. 2025. PMID: 40369462 Free PMC article.
-
Association of triglyceride-glucose index and traditional risk factors with cardiovascular disease among non-diabetic population: a 10-year prospective cohort study.Cardiovasc Diabetol. 2022 Nov 24;21(1):256. doi: 10.1186/s12933-022-01694-3. Cardiovasc Diabetol. 2022. PMID: 36434636 Free PMC article.
References
-
- Kivimaki M, Kuosma E, Ferrie JE, Luukkonen R, Nyberg ST, Alfredsson L, et al. . Overweight, obesity, and risk of cardiometabolic multimorbidity: pooled analysis of individual-level data for 120–813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health. (2017) 2:e277–e85. doi: 10.1016/S2468-2667(17)30074-9 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous