

Evaluation of Immediate Postpartum Long-Acting Reversible Contraception for Reducing Short-Interval Pregnancies
- PMID: 40458344
- PMCID: PMC12128560
- DOI: 10.7759/cureus.83395
Evaluation of Immediate Postpartum Long-Acting Reversible Contraception for Reducing Short-Interval Pregnancies
Abstract
Background: Short interpregnancy intervals (conception occurring <18 months after delivery or pregnancy loss) are associated with increased risk of adverse outcomes such as preterm delivery, low birth weight, and invasive placental pathologies. To reduce unintended short-interval pregnancy (SIP) among people desiring contraception, our health network in 2019 began offering immediate postpartum long-acting reversible contraception (LARC), using copper and hormonal intrauterine devices (IUDs) and etonogestrel implants. This study evaluated the impact of the initiative on the incidence of SIP at our institution.
Methods: We conducted a retrospective cohort study of patients on government insurance who delivered between July 1, 2019, and March 31, 2020. The exposure of interest was LARC placement in the immediate postpartum period. The outcome of interest was confirmed pregnancy within 18 months of delivery. Exclusion criteria were immediate postpartum sterilization, cesarean or peripartum hysterectomy, or fetal demise. SIP rates were compared between those opting for LARC immediately after delivery (pp LARC group) and those who declined (no pp LARC group). A logistic regression model controlled for potential confounders.
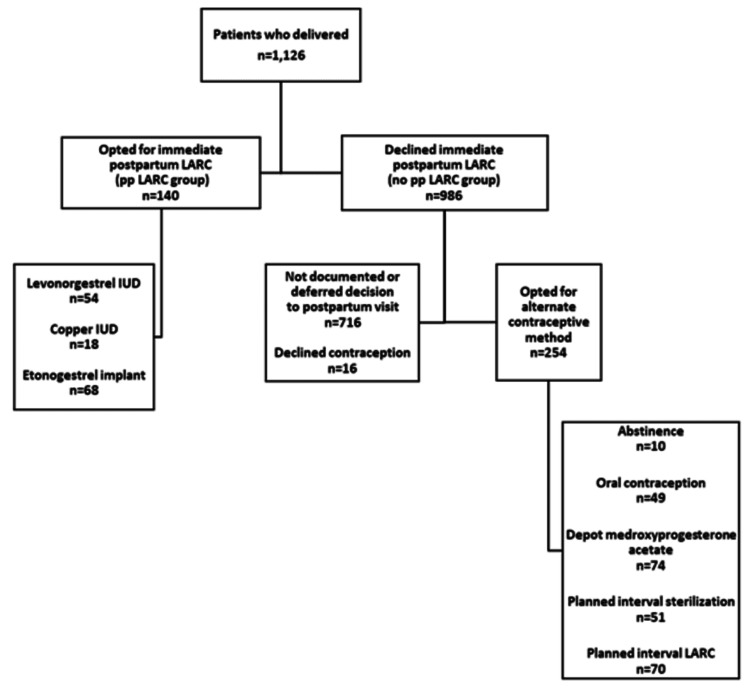
Results: Of the 1,126 patients who met the inclusion criteria, there were 140 in the pp LARC group (68 etonogestrel implant, 54 levonorgestrel IUD, and 18 copper IUD) and 986 in the no pp LARC group. The pp LARC group experienced a lower proportion of SIP (7.9% versus 23.8%, P < 0.001). In adjusted analysis, immediate postpartum LARC reduced the rate of SIP (adjusted risk ratio (ARR): 0.28, 95% confidence interval (CI): 0.14-0.55, P < 0.001).
Conclusion: Providing LARC shortly after delivery shows promise for patient uptake and prevention of SIP among individuals wishing for contraception. Expanded studies are warranted.
Keywords: birth intervals; long-acting reversible contraception; postpartum contraception; pregnancy outcome; short interpregnancy interval.
Copyright © 2025, Grover et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Lehigh Valley Health Network issued approval IRB00001409. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Associations between immediate postpartum long-acting reversible contraception and short interpregnancy intervals.Contraception. 2020 Dec;102(6):409-413. doi: 10.1016/j.contraception.2020.08.016. Epub 2020 Sep 10. Contraception. 2020. PMID: 32918870
-
The effects of offering immediate postpartum placement of IUDs and implants to pregnant patients with heart disease.Contraception. 2022 Jan;105:55-60. doi: 10.1016/j.contraception.2021.09.005. Epub 2021 Sep 14. Contraception. 2022. PMID: 34529951
-
Postpartum contraception: initiation and effectiveness in a large universal healthcare system.Am J Obstet Gynecol. 2017 Jul;217(1):55.e1-55.e9. doi: 10.1016/j.ajog.2017.02.036. Epub 2017 Feb 28. Am J Obstet Gynecol. 2017. PMID: 28257962
-
Immediate postpartum provision of long-acting reversible contraception.Curr Opin Obstet Gynecol. 2015 Dec;27(6):460-4. doi: 10.1097/GCO.0000000000000224. Curr Opin Obstet Gynecol. 2015. PMID: 26536209 Review.
-
Patients and providers' knowledge, attitudes, and beliefs regarding immediate postpartum long-acting reversible contraception: a systematic review.Women Health. 2020 Feb;60(2):179-196. doi: 10.1080/03630242.2019.1616042. Epub 2019 May 23. Women Health. 2020. PMID: 31122167
References
-
- Obstetric Care Consensus No. 8: Interpregnancy care. Obstet Gynecol. 2019;133:0–72. - PubMed
-
- Interpregnancy interval and adverse pregnancy outcomes: an analysis of successive pregnancies. Hanley GE, Hutcheon JA, Kinniburgh BA, Lee L. Obstet Gynecol. 2017;129:408–415. - PubMed
-
- Short interval pregnancy is associated with pathology severity in placenta accreta spectrum (PAS) Munoz JL, Hernandez B, Ireland KE, Ramsey PS. J Matern Fetal Neonatal Med. 2022;35:8863–8868. - PubMed
-
- Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. JAMA. 2006;295:1809–1823. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous