

Clinical Features and Natural Progression of Unilateral High Myopia in Adults: A Comparison Study
- PMID: 40458669
- PMCID: PMC12127622
- DOI: 10.1016/j.xops.2025.100780
Clinical Features and Natural Progression of Unilateral High Myopia in Adults: A Comparison Study
Abstract
Purpose: To investigate and compare the clinical characteristics of patients with unilateral high myopia (UHM) and bilateral high myopia (BHM) based on axial length (AL).
Design: A retrospective cohort study.
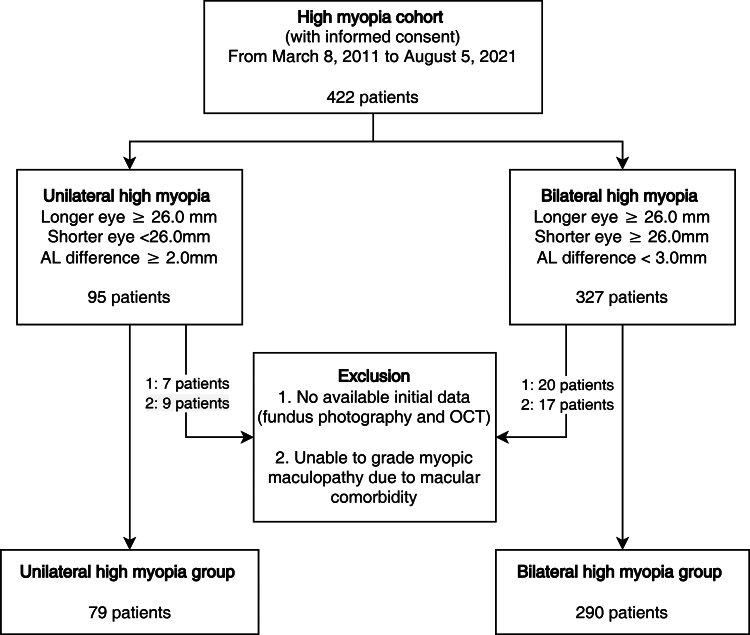
Participants: Adult patients diagnosed with UHM or BHM between March 2011 and August 2021.
Methods: Unilateral high myopia was defined as ≥26 mm AL in 1 eye and <26 mm in the other, with ≥2 mm difference. Bilateral high myopia was defined as ≥26 mm AL in both eyes, with ≤3 mm difference. In each patient, the eye with the longer AL was designated the "longer eye" and the other the "shorter eye." We analyzed differences in clinical features, including ophthalmic history, best-corrected visual acuity, ocular biometry, and myopic maculopathy grade. Myopic maculopathy was graded based on atrophy, traction, and neovascularization using a known method. Long-term features included treatments for myopic neovascular maculopathy and myopic tractional maculopathy and AL change over time.
Main outcome measures: Comparison of clinical characteristics between UHM and BHM groups.
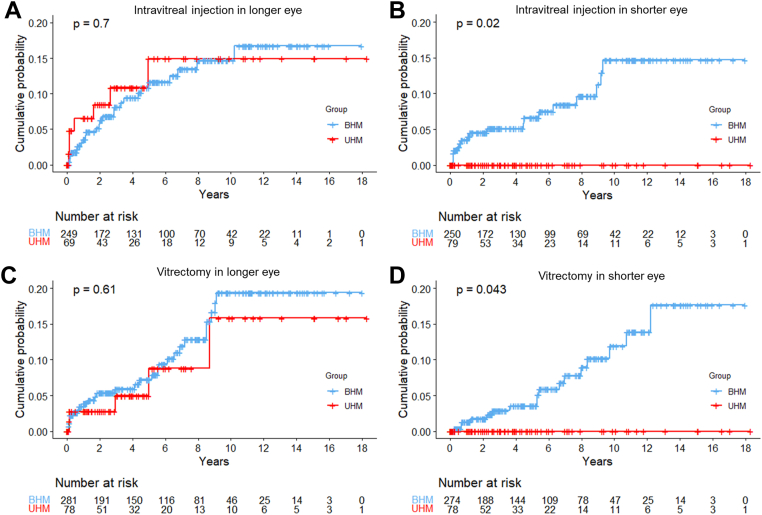
Results: We analyzed 369 patients (79 with UHM and 290 with BHM) with a median follow-up period of 4.5 years. The UHM group had a higher proportion of women than the BHM group (88.8% vs. 76.2%, P = 0.025). Compared with longer eyes in the BHM group, those in the UHM group had worse best-corrected visual acuity (0.8 ± 0.6 vs. 0.6 ± 0.6 in logarithm of the minimum angle of resolution, P < 0.001) despite having shorter AL (29.1 ± 1.6 mm vs. 30.6 ± 1.9 mm, P < 0.001). In the analysis of AL changes, shorter eyes in the UHM group showed no elongation over time (0.014 mm/year, P = 0.12), unlike the longer eyes in UHM and both eyes in BHM (0.049-0.071 mm/year, P < 0.01).
Conclusions: Adult UHM patients mostly lacked associated environmental factors. The poorer visual acuity in the longer eyes of UHM patients, which cannot be explained by structural abnormalities, suggests that the interocular difference may have originated in early childhood. During the follow-up period, AL elongation and myopic complications occurred at similar rates in the longer eye of UHM and both eyes of BHM. Meanwhile, such changes were not observed in the shorter eye in UHM. Further investigation of the underlying mechanisms, such as the genetic factors contributing to this extreme asymmetry, is warranted.
Financial disclosures: The author(s) have no proprietary or commercial interest in any materials discussed in this article.
Keywords: Bilateral high myopia; Myopic maculopathy; Ocular asymmetry; Unilateral high myopia.
© 2025 by the American Academy of Ophthalmologyé.
Figures

Similar articles
-
Three-Dimensional Eye Shape, Myopic Maculopathy, and Visual Acuity: The Zhongshan Ophthalmic Center-Brien Holden Vision Institute High Myopia Cohort Study.Ophthalmology. 2017 May;124(5):679-687. doi: 10.1016/j.ophtha.2017.01.009. Epub 2017 Feb 23. Ophthalmology. 2017. PMID: 28237427
-
Progression of Myopic Maculopathy during 18-Year Follow-up.Ophthalmology. 2018 Jun;125(6):863-877. doi: 10.1016/j.ophtha.2017.12.005. Epub 2018 Jan 19. Ophthalmology. 2018. PMID: 29371011
-
Inter-Eye Comparison in Highly Myopic Patients with Unilateral Myopic Traction Maculopathy.Curr Eye Res. 2022 Apr;47(4):642-649. doi: 10.1080/02713683.2021.2009517. Epub 2021 Dec 14. Curr Eye Res. 2022. PMID: 34903124
-
Tessellated fundus appearance and its association with myopic refractive error.Clin Exp Optom. 2019 Jul;102(4):378-384. doi: 10.1111/cxo.12822. Epub 2018 Aug 9. Clin Exp Optom. 2019. PMID: 30091794
-
Prevalence of Myopic Macular Features in Dutch Individuals of European Ancestry With High Myopia.JAMA Ophthalmol. 2022 Feb 1;140(2):115-123. doi: 10.1001/jamaophthalmol.2021.5346. JAMA Ophthalmol. 2022. PMID: 34913968 Free PMC article.
References
-
- Pararajasegaram R. VISION 2020-the right to sight: from strategies to action. Am J Ophthalmol. 1999;128:359–360. - PubMed
-
- Vitale S., Sperduto R.D., Ferris F.L., 3rd Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Arch Ophthalmol. 2009;127:1632–1639. - PubMed
-
- Holden B.A., Fricke T.R., Wilson D.A., et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036–1042. - PubMed
-
- Silva R. Myopic maculopathy: a review. Ophthalmologica. 2012;228:197–213. - PubMed
-
- Ohno-Matsui K. What is the fundamental nature of pathologic myopia? Retina. 2017;37:1043–1048. - PubMed
LinkOut - more resources
Full Text Sources
