

Immunohistochemical evaluation of a trial of gantenerumab or solanezumab in dominantly inherited Alzheimer disease
- PMID: 40459787
- PMCID: PMC12133910
- DOI: 10.1007/s00401-025-02890-7
Immunohistochemical evaluation of a trial of gantenerumab or solanezumab in dominantly inherited Alzheimer disease
Abstract
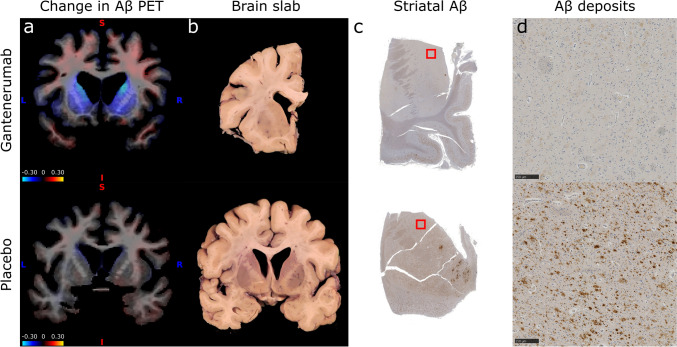
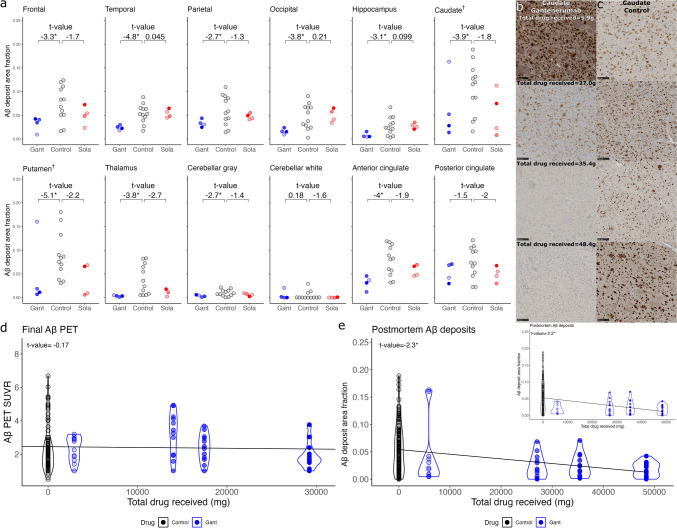
Clinical trials of anti-amyloid-β (Aβ) monoclonal antibodies in Alzheimer disease (AD) infer target engagement from Aβ positron emission tomography (PET) and/or fluid biomarkers such as cerebrospinal fluid (CSF) Aβ42/40. However, these biomarkers measure brain Aβ deposits indirectly and/or incompletely. In contrast, neuropathologic assessments allow direct investigation of treatment effects on brain Aβ deposits-and on potentially myriad 'downstream' pathologic features. From a clinical trial of anti-Aβ monoclonal antibodies in dominantly inherited AD (DIAD), in the largest study of its kind, we measured immunohistochemistry area fractions (AFs) for Aβ deposits (10D5), tauopathy (PHF1), microgliosis (IBA1), and astrocytosis (GFAP) in 10 brain regions from 10 trial cases-gantenerumab (n = 4), solanezumab (n = 4), placebo/no treatment (n = 2)-and 10 DIAD observational study cases. Strikingly, in proportion to total drug received, Aβ deposit AFs were significantly lower in the gantenerumab arm versus controls in almost all areas examined, including frontal, temporal, parietal, and occipital cortices, anterior cingulate, hippocampus, caudate, putamen, thalamus, and cerebellar gray matter; only posterior cingulate and cerebellar white matter comparisons were non-significant. In contrast, AFs of tauopathy, microgliosis, and astrocytosis showed no differences across groups. Our results demonstrate with direct histologic evidence that gantenerumab treatment in DIAD can reduce parenchymal Aβ deposits throughout the brain in a dose-dependent manner, suggesting that more complete removal may be possible with earlier and more aggressive treatment regimens. Although AFs of tauopathy, microgliosis, and astrocytosis showed no clear response to partial Aβ removal in this limited autopsy cohort, future examination of these cases with more sensitive techniques (e.g., mass spectrometry) may reveal more subtle 'downstream' effects.
Keywords: Alzheimer disease; Anti-amyloid-β monoclonal antibodies; CSF; Clinical trial; Digital pathology; PiB PET.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Washington University holds patents for one of the treatments (solanezumab), previously tested in the DIAN clinical trials. If solanezumab is approved as a treatment for Alzheimer’s disease or Dominantly Inherited Alzheimer’s Disease, Washington University will receive part of the net sales of solanezumab from Eli Lilly, which has licensed the patents related to solanezumab from Washington University. Johannes Levin reports speaker fees from Bayer Vital, Biogen, EISAI, TEVA, Zambon, Merck and Roche, consulting fees from Axon Neuroscience, EISAI and Biogen, author fees from Thieme medical publishers and W. Kohlhammer GmbH medical publishers and is inventor in a patent “Oral Phenylbutyrate for Treatment of Human 4-Repeat Tauopathies” (EP 23 156 122.6) filed by LMU Munich. In addition, he reports compensation for serving as chief medical officer for MODAG GmbH, is beneficiary of the phantom share program of MODAG GmbH and is inventor in a patent “Pharmaceutical Composition and Methods of Use” (EP 22 159 408.8) filed by MODAG GmbH, all activities outside the submitted work. Tammie Benzinger, MD, PhD, has received investigator initiated research funding from the NIH, the Alzheimer’s Association, the Foundation at Barnes-Jewish Hospital, Siemens Healthineers and Avid Radiopharmaceuticals (a wholly-owned subsidiary of Eli Lilly and Company). She participates as a site investigator in clinical trials sponsored by Eli Lilly and Company, Biogen, Eisai, Jaansen, and Roche. She has served as a paid and unpaid consultant to Eisai, Siemens, Biogen, Janssen, and Bristol-Myers Squibb. John Morris consults for Barcelonaβeta Brain Research Foundation Scientific Advisory Board and Diverse VCID Observational Study Monitoring Board. He is on the advisory board for Cure Alzheimer’s Fund Research Strategy Council and LEADS Advisory Board, University of Indiana. John Morris is funded by NIH grants # P30 AG066444; P01AG003991; P01AG026276. Neither John Morris nor his family owns stock or has equity interest (outside of mutual funds or other externally directed accounts) in any pharmaceutical or biotechnology company. Sandra Black reports grants or contracts from any entity (Contract Research: Genentech, Optina, Roche, Eli Lilly, Eisa/Biogen Idec, NovoNordisk, Lilly Avid, ICON; Peer Reviewed: Ontario Brain Institute, CIHR, Leducq Foundation, Heart and Stroke Foundation of Canada, NIH, Alzheimer’s Drug Discovery Foundation, Brain Canada, Weston Brain Institute, Canadian Partnership for Stroke Recovery, Canadian Foundation for Innovation, Focused Ultrasound Foundation, Alzheimer’s Association US, Department of National Defence, Montreal Medical International Kuwait, Queen’s University, Compute Canada Resources for Research Groups, CANARIE, Networks of Centres of Excellence of Canada), consulting fees (Roche, Biogen, NovoNordisk, Eisai, Eli Lilly), payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events (Biogen, Roche New England Journal Manuscript, Roche Models of Care Analysis in Canada in Submission, Eisai MRI Workshop), and participation on a Data Safety Monitoring Board or Advisory Board (Conference Board of Canada, World Dementia Council, University of Rochester Contribution to the Mission and Scientific Leadership of the Small Vessel VCID Biomarker Validation Consortium, National Institute of Neurological Disorders and Stroke). Lawrence Honig has received funding for consulting from Biogen, Eisai, Genentech/Roche, Medscape, and Prevail/Lilly, and has received institutional research funding from Abbvie, Acumen, Alector, AstraZeneca, Axovant, Avanir, Biogen, Bristol-Myer Squibb, Cognition, EIP, Eisai, Genentech/Roche, Janssen/Johnson & Johnson, Eli Lilly, Merck, Transposon, UCB, and Vaccinex. Richard Perrin’s laboratory receives cost recovery funding from Biogen for tissue procurement and processing services related to ALS clinical trials. Ethical approval: The study was conducted in accordance with the Declaration of Helsinki (version 7) and the International Conference on Harmonization and Good Clinical Practice guidelines. Protocols for the study have received prior approval by the local Institutional Review Board (IRB) or Ethics Committee of each DIAN site and by the Washington University IRB for the Knight ADRC. The clinical trial registration number is NCT01760005.
Figures

References
-
- Andersson E, Lindblom N, Janelidze S, Salvadó G, Gkanatsiou E, Söderberg L et al (2025) Soluble cerebral Aβ protofibrils link Aβ plaque pathology to changes in CSF Aβ42/Aβ40 ratios, neurofilament light and tau in Alzheimer’s disease model mice. Nat Aging 5:366–375. 10.1038/s43587-025-00810-8 - DOI - PMC - PubMed
-
- Barthélemy NR, Toth B, Manser PT, Sanabria-Bohórquez S, Teng E, Keeley M et al (2022) Site-specific cerebrospinal fluid tau hyperphosphorylation in response to alzheimer’s disease brain pathology: not all tau phospho-sites are hyperphosphorylated. J Alzheimer’s Dis 85:415–429. 10.3233/JAD-210677 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K01 AG080123/AG/NIA NIH HHS/United States
- P30 AG066444/AG/NIA NIH HHS/United States
- U19AG032438/NH/NIH HHS/United States
- R01 AG053267/AG/NIA NIH HHS/United States
- S10 RR027552/RR/NCRR NIH HHS/United States
- K01 AG084816/AG/NIA NIH HHS/United States
- T32 AG058518/AG/NIA NIH HHS/United States
- R01 AG052550/AG/NIA NIH HHS/United States
- P30 NS098577/NS/NINDS NIH HHS/United States
- P30 NS057105/NS/NINDS NIH HHS/United States
- U01 AG042791/AG/NIA NIH HHS/United States
- U19 AG032438/AG/NIA NIH HHS/United States
- P30 AG066468/AG/NIA NIH HHS/United States
- P01 AG003991/AG/NIA NIH HHS/United States
- R01 AG046179/AG/NIA NIH HHS/United States
- R01 AG068319/AG/NIA NIH HHS/United States
- P01 AG026276/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
