

A white matter-centered approach to investigate recurrence pathways in high-grade gliomas: a single-center retrospective study
- PMID: 40459831
- PMCID: PMC12198263
- DOI: 10.1007/s11060-025-05050-9
A white matter-centered approach to investigate recurrence pathways in high-grade gliomas: a single-center retrospective study
Abstract
Background and aim: High-grade gliomas (HGGs) are aggressive primary brain tumors with inevitable recurrence. This single-center retrospective study investigates whether the anatomical proximity of HGGs to major white matter tracts influences progression and recurrence. The study explores the association between tumor location and recurrence type-local, remote, or ependymal-and whether recurrences align with adjacent white matter tracts.
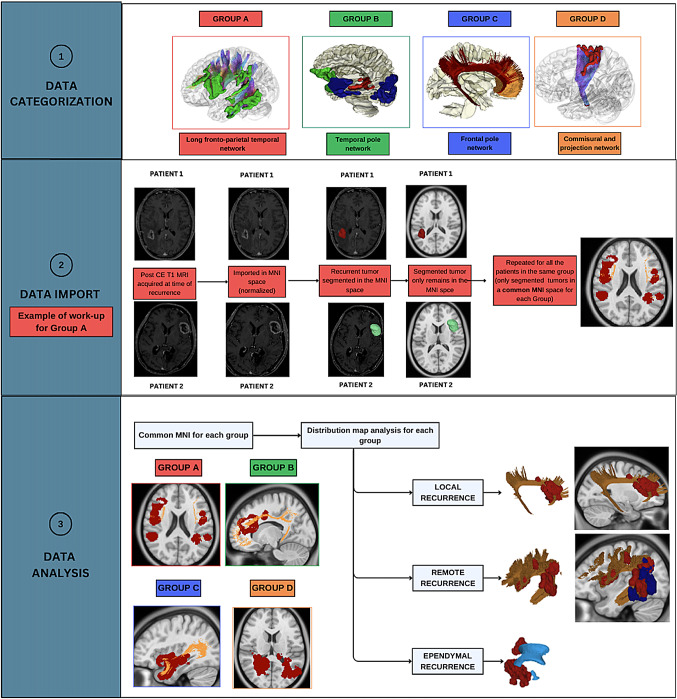
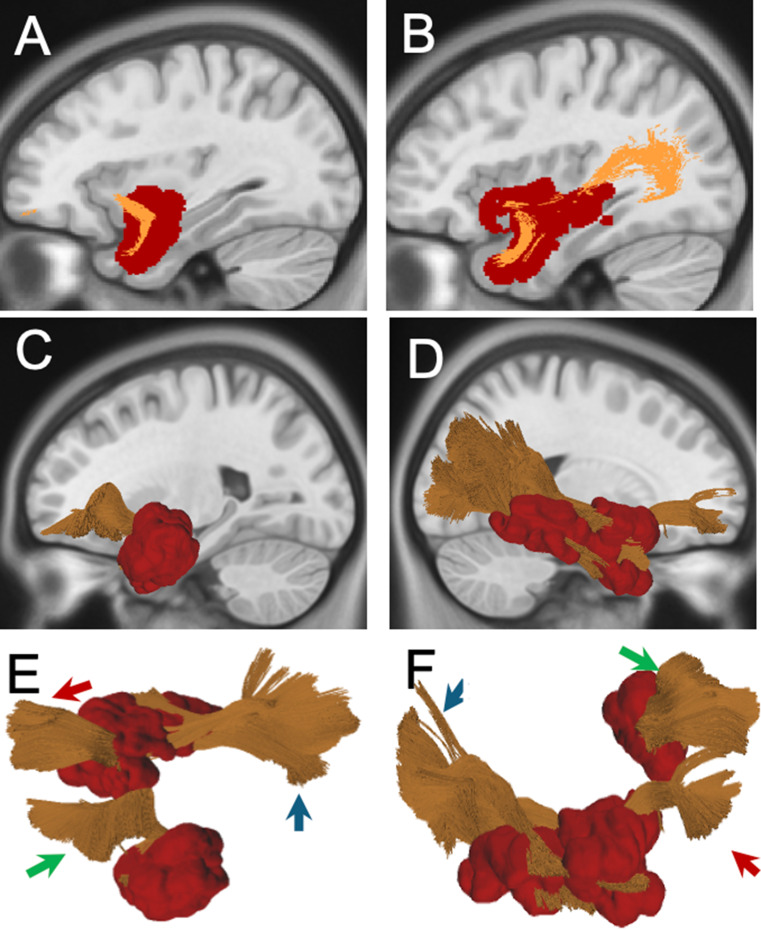
Methods: The study included patients with histopathologically confirmed recurrent HGGs who underwent reoperation. Primary tumors were categorized into four anatomical subgroups using a connectivity-based framework from the HCP 1065 Atlas: Subgroup A: Long Fronto-Temporo-Parietal Network Subgroup B: Temporal Pole Network (further divided into B1, B2, and B3 based on connectivity patterns) Subgroup C: Frontal Pole Network Subgroup D: Commissural and Projection Networks (further divided into D1 and D2). Recurrences were classified via post-contrast T1-weighted MRI as local, remote, ependymal. The Tract-to-Region Connectome (T-R-C) assessed the volumetric overlap between recurrence maps and main white matter bundles.
Results: Of 41 patients, a significant correlation emerged between tumor subgroup and recurrence type (p = 0.0003). Subgroup A predominantly showed remote recurrences (68%), while B2, B3, C, and D2 had mainly local recurrences. Subgroup D1 had a predominance of ependymal recurrences (66.7%). Local and remote recurrences largely conformed to adjacent white matter distributions, with variations in timing of recurrence and survival observed across different groups.
Conclusion: Our analysis, focused on exploring the spatial aspects of recurrence in relation to white matter anatomy, suggests that HGG recurrence patterns are strongly influenced by anatomical location and white matter architecture. Certain anatomical areas show a predisposition toward specific recurrence patterns. Recognizing these spatial dynamics may guide more precise surgical strategies, radiotherapy targeting, and recurrence risk assessment.
Keywords: High grade glioma; Recurrence; White matter.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The Institutional Review Board (IRB) of Fondazione Policlinico Gemelli IRCCS approved this study (ID 7028). Competing interests: The authors declare no competing interests.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
