

Association of physician-delivered virtual care near the end of life with healthcare use outcomes: A national population-based study of Canadians
- PMID: 40460327
- PMCID: PMC12133171
- DOI: 10.1371/journal.pone.0324898
Association of physician-delivered virtual care near the end of life with healthcare use outcomes: A national population-based study of Canadians
Abstract
Background: The last 90 days of life are marked by high healthcare utilization in acute care settings, often conflicting with the preference to remain at home. The COVID-19 pandemic accelerated the adoption of virtual care, but its impact on healthcare utilization near the end-of-life remains unclear. This study assessed the association between physician-delivered virtual care use near the end-of-life and acute healthcare utilization, before and during the COVID-19 pandemic across four Canadian provinces.
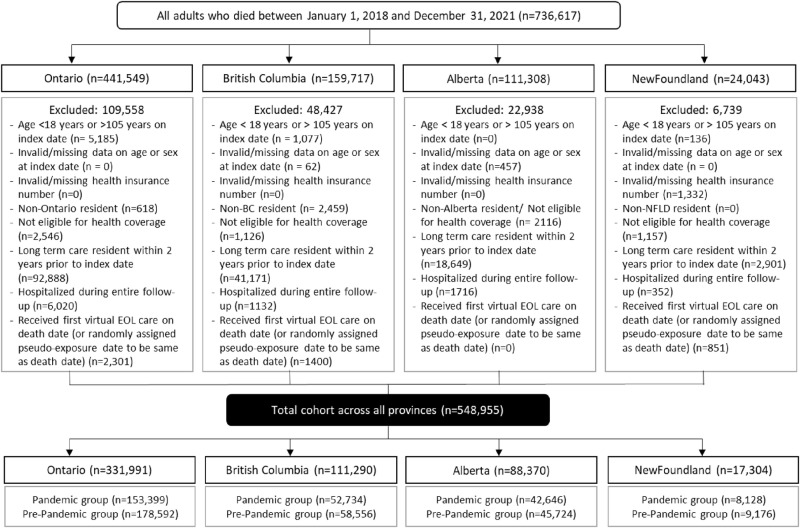
Methods: A retrospective population-based cohort study using linked health administrative data from January 1, 2018, to December 31, 2021, across British Columbia (BC), Alberta (AB), Ontario (ON), and Newfoundland & Labrador (NFLD). The study included 548,955 adult decedents who died within the study period. Virtual care use in the last 90 days of life, categorized by pre-pandemic and pandemic periods, was the primary exposure. Primary outcomes were rates of ED visits, hospitalizations, and in-hospital deaths during the last 90 days of life. Modified Poisson regression models were used to measure associations, adjusting for demographic and clinical characteristics.
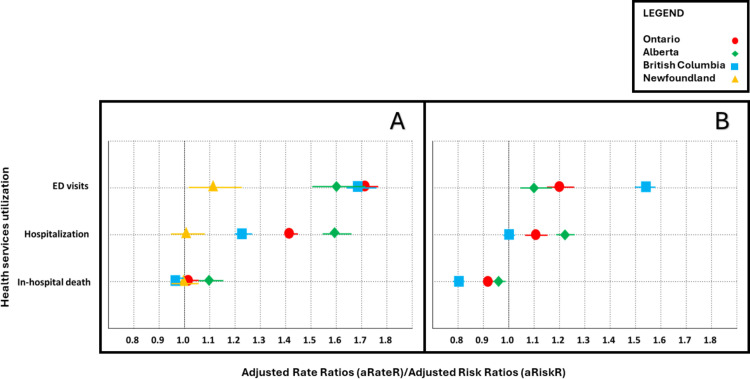
Results: Among the 548,955 decedents, virtual care utilization during the pandemic varied by province, ranging from 53% in NFLD to 78% in BC. During the pandemic, virtual care was associated with higher ED visits (adjusted rate ratios [aRateRs] ranging from 1.12 to 1.72) and hospitalizations (aRateRs: ranging from 1.01 to 1.59) in most provinces. Virtual care was linked to a higher risk of in-hospital death in AB (adjusted risk ratios [aRiskR]: 1.11; 95% CI: 1.08-1.14; P < 0.001) and ON (aRiskR: 1.04; 95% CI: 1.03-1.05; P < 0.001). Pre-pandemic, associations were weaker, with virtual care linked to lower in-hospital death rates in ON, AB and BC.
Conclusion: Virtual care during the pandemic was linked to increased acute healthcare utilization, contrasting with pre-pandemic patterns when it appeared more selective and associated with fewer in-hospital deaths. Findings highlight the evolving role of virtual care and the need for region-specific policies to optimize end-of-life care delivery.
Copyright: © 2025 Anwar et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Comparison of physician-delivered models of virtual and home-based in-person care for adults in the last 90 days of life with cancer and terminal noncancer illness during the COVID-19 pandemic.PLoS One. 2024 Nov 27;19(11):e0301813. doi: 10.1371/journal.pone.0301813. eCollection 2024. PLoS One. 2024. PMID: 39602394 Free PMC article.
-
Population-Based Estimates of Health Care Utilization and Expenditures by Adults During the Last 2 Years of Life in Canada's Single-Payer Health System.JAMA Netw Open. 2020 Apr 1;3(4):e201917. doi: 10.1001/jamanetworkopen.2020.1917. JAMA Netw Open. 2020. PMID: 32236531 Free PMC article.
-
Use of virtual care near the end of life before and during the COVID-19 pandemic: A population-based cohort study.PLoS One. 2025 Jan 8;20(1):e0313766. doi: 10.1371/journal.pone.0313766. eCollection 2025. PLoS One. 2025. PMID: 39774523 Free PMC article.
-
Visitor Restrictions During the COVID-19 Pandemic and Increased Falls With Harm at a Canadian Hospital: An Exploratory Study.J Patient Saf. 2024 Sep 1;20(6):434-439. doi: 10.1097/PTS.0000000000001237. Epub 2024 Jun 26. J Patient Saf. 2024. PMID: 38917342
-
Nurse practitioner and physician end-of-life home visits and end-of-life outcomes.BMJ Support Palliat Care. 2024 Dec 19;14(e3):e2761-e2769. doi: 10.1136/spcare-2023-004392. BMJ Support Palliat Care. 2024. PMID: 37979954 Free PMC article.
References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
