

Evaluating the Potential of COL8A1 as a Therapeutic Target for Chemoresistance, Disease Progression, and a Prognostic Marker in Gastric Cancer
- PMID: 40461943
- PMCID: PMC12133449
- DOI: 10.1111/jcmm.70621
Evaluating the Potential of COL8A1 as a Therapeutic Target for Chemoresistance, Disease Progression, and a Prognostic Marker in Gastric Cancer
Abstract
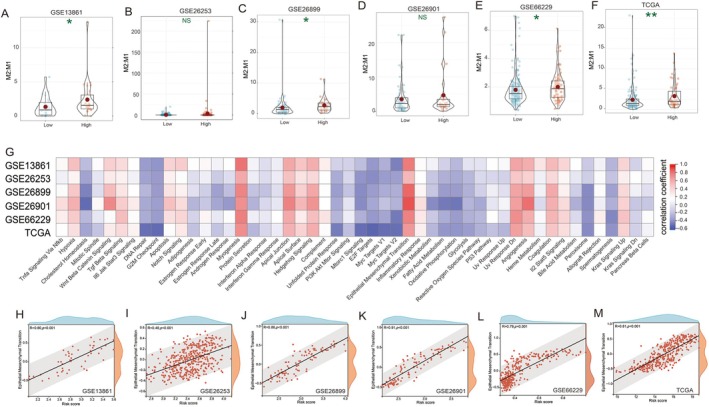
This study aimed to identify key genes associated with post-chemotherapy recurrence in gastric cancer patients. Gene expression data from multiple cohorts were analysed to determine differentially expressed genes between recurrent and non-recurrent cases. A prognostic risk model incorporating COL8A1, HSPB7 and SLIT2 was developed and validated across six independent cohorts. The risk score demonstrated significant associations with disease-free and overall survival, tumour grade and molecular subtypes. Notably, the risk score showed potential as a predictor of immunotherapy response, outperforming established markers such as microsatellite instability score and Epstein-Barr virus status. Analysis of the tumour immune microenvironment revealed a correlation between risk score and M2 macrophage infiltration. A nomogram integrating the risk score with clinical factors demonstrated high accuracy in predicting patient survival. Further investigation of COL8A1 revealed its significant role in gastric cancer cell proliferation, metastasis, and chemoresistance. In vitro and in vivo experiments showed that COL8A1 knockdown inhibited cancer cell growth, invasion, and metastasis while enhancing chemosensitivity. These findings provide valuable insights into the molecular mechanisms of gastric cancer recurrence and offer potential biomarkers for prognosis and treatment response prediction. The study highlights the importance of integrating genomic data with clinical information to improve patient stratification and personalised treatment strategies in gastric cancer management.
Keywords: COL8A1; chemotherapy; gastric cancer; immunotherapy; recurrence.
© 2025 The Author(s). Journal of Cellular and Molecular Medicine published by Foundation for Cellular and Molecular Medicine and John Wiley & Sons Ltd.
Conflict of interest statement
Animal Studies: Experimentation on zebrafish larvae younger than 5 days old does not require ethics committee approval. Our study adhered to ARRIVE guidelines for reporting animal research.
The authors declare no conflicts of interest.
Figures






Similar articles
-
COL8A1 is a potential prognostic biomarker associated with migration, proliferation, and tumor microenvironment in glioma.Exp Cell Res. 2024 Jun 1;439(1):114076. doi: 10.1016/j.yexcr.2024.114076. Epub 2024 May 7. Exp Cell Res. 2024. PMID: 38719174
-
The necroptosis-related signature and tumor microenvironment immune characteristics associated with clinical prognosis and drug sensitivity analysis in stomach adenocarcinoma.Aging (Albany NY). 2024 Mar 27;16(7):6098-6117. doi: 10.18632/aging.205690. Epub 2024 Mar 27. Aging (Albany NY). 2024. PMID: 38546403 Free PMC article.
-
Single-cell analysis uncovers high-proliferative tumour cell subtypes and their interactions in the microenvironment of gastric cancer.J Cell Mol Med. 2024 Jun;28(12):e18373. doi: 10.1111/jcmm.18373. J Cell Mol Med. 2024. PMID: 38894657 Free PMC article.
-
Construction of a prognostic model for gastric cancer based on immune infiltration and microenvironment, and exploration of MEF2C gene function.BMC Med Genomics. 2025 Jan 14;18(1):13. doi: 10.1186/s12920-024-02082-4. BMC Med Genomics. 2025. PMID: 39810215 Free PMC article.
-
Dysregulation of miRNAs as a signature for diagnosis and prognosis of gastric cancer and their involvement in the mechanism underlying gastric carcinogenesis and progression.IUBMB Life. 2020 May;72(5):884-898. doi: 10.1002/iub.2259. Epub 2020 Feb 20. IUBMB Life. 2020. PMID: 32078236 Review.
References
-
- Alsina M., Arrazubi V., Diez M., and Tabernero J., “Current Developments in Gastric Cancer: From Molecular Profiling to Treatment Strategy,” Nature Reviews. Gastroenterology & Hepatology 20 (2023): 155–170. - PubMed
MeSH terms
Substances
Grants and funding
- 2021Y9022/Joint Funds for the Innovation of Science and Technology, Fujian province:
- 2021QNA001/Fujian provincial health technology project
- 2023J011166/Natural Science Foundation of Fuiian Province
- X2024037/Fujian University of Traditional Chinese Medicine
- 2023Y9292/Joint Funds for the Innovation of Science and Technology Fuiian province
LinkOut - more resources
Full Text Sources
Medical
