

Associations of aortic and carotid artery health with cerebrovascular markers and cognition in older adults from the Whitehall II imaging study
- PMID: 40462085
- PMCID: PMC12135225
- DOI: 10.1186/s12916-025-04105-y
Associations of aortic and carotid artery health with cerebrovascular markers and cognition in older adults from the Whitehall II imaging study
Abstract
Background: Cardiovascular disease has been associated with an increased dementia risk, but the underlying mechanisms for this heart-brain link are unclear. This study sought to examine associations between aortic and carotid artery structure with cerebrovascular reactivity (CVR), white matter hyperintensities (WMHs), and cognition in later-life.
Methods: One hundred sixty three participants (25.8% female) from the Whitehall II Imaging cohort completed two examinations (M ± SD age 68.2 ± 4.4 at Wave-1 and 76.9 ± 4.5 at Wave-2) of neuropsychological assessments and 3T brain magnetic resonance imaging (MRI) FLAIR scans to quantify WMHs. Wave-2 additionally included vascular sonography of the aorta and carotid artery, and 3T functional MRI scans to measure CVR (mean % change BOLD signal change during a CO2 challenge). Wave-2 factor scores of aortic and carotid arterial diameters, stiffness, and compliance were the exposure variables. Midlife Framingham Cardiovascular Risk Score (FRS) measured before Wave-1 was a potential effect modifier. WMH volume, grey matter CVR, cognitive factor scores (episodic memory, working memory, executive function, visuospatial memory, fluency, lexical retrieval) at Wave-2, and changes in WMH and cognition between Wave-1 and Wave-2 were used as outcome variables.
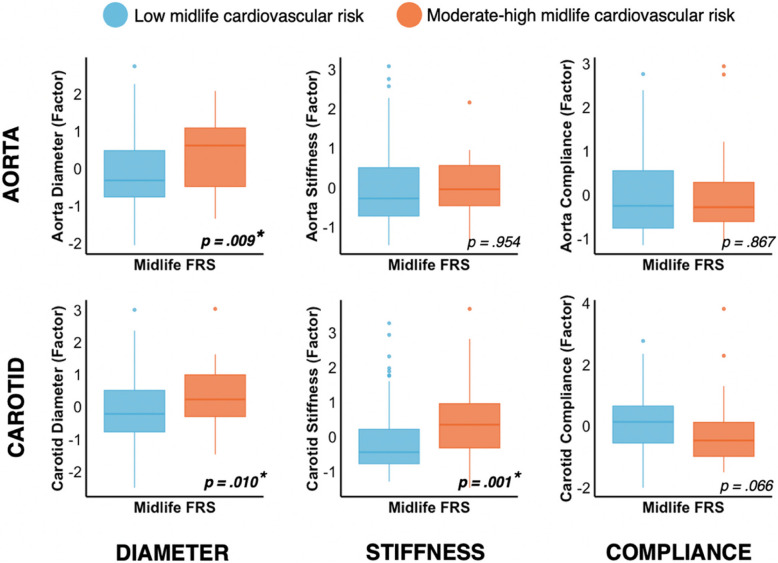
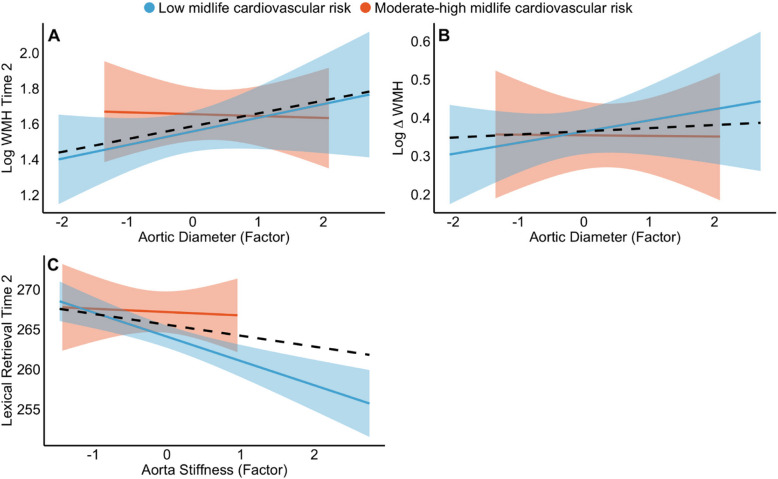
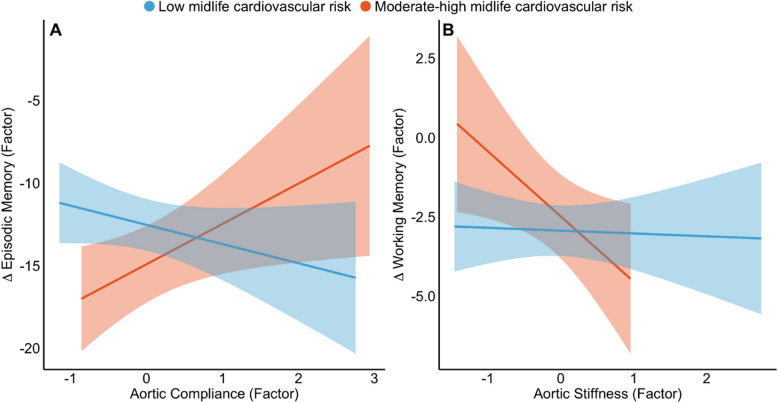
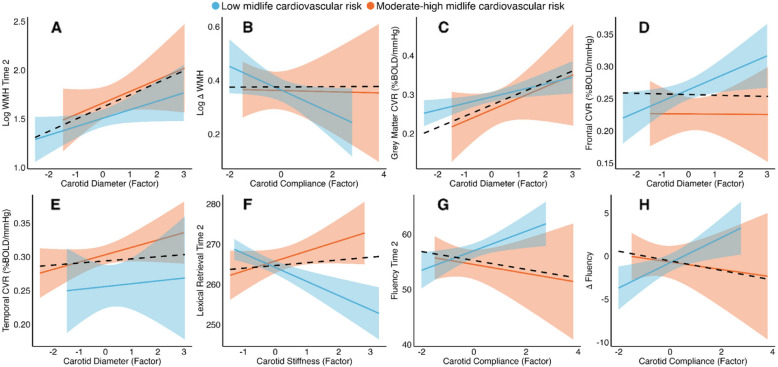
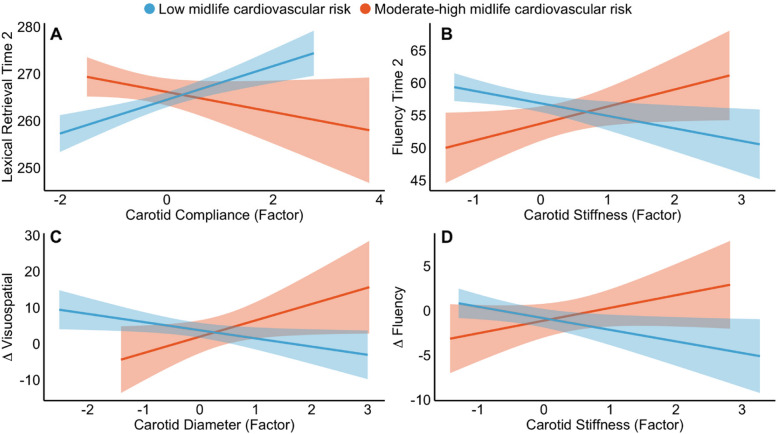
Results: Larger aortic diameter (ß = 0.38, SE = 0.11) and greater aortic stiffness (ß = 0.27, SE = 0.10) were associated with larger carotid diameter, independently of body size. Higher midlife FRS was associated with larger aortic and carotid diameters and increased carotid stiffness in old age. We observed notable artery-brain associations, such that larger aortic (ß = 0.17, SE = 0.06) and carotid diameters (ß = 0.11, SE = 0.05) were associated with larger WMH lesion volumes at Wave-2. Larger aortic diameter (ß = 0.08 SE = 0.03) and lower carotid compliance (ß = - 0.06, SE = 0.02) at Wave-2 were also associated with greater longitudinal increases in WMH volumes over the preceding 9 years. Higher stiffness and lower compliance of the aorta and carotid were associated with worse cognitive outcomes across a range of domains, and these associations were moderated by midlife FRS. Larger carotid diameter was associated with higher cerebrovascular reactivity (ß = 0.02, SE = 0.01), suggesting a potential compensatory pathway.
Conclusions: Adverse structural and functional changes in the aorta and carotid artery were inter-related and associated with vascular brain lesions, cerebrovascular reactivity, and poorer cognitive outcomes in older age.
Keywords: Aorta; Cardiovascular risk factors; Carotid; Cognition; Dementia; Longitudinal cohort; Magnetic resonance imaging; Ultrasound.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study complied with the relevant international and domestic ethical guidelines and was approved by the University of Oxford at MRI-Wave-1 (2012–2016, MSD/IDREC/2010/P17.2) and MRI-Wave-2 (2019–2023; R57135/RE006). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Yu R, Lui F. Neuroanatomy, brain arteries. Treasure Island (FL): StatPearls; 2022. [updated 2022; cited 2025 May 7]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549894/. - PubMed
MeSH terms
Grants and funding
- SBF006\1078/BHF_/British Heart Foundation/United Kingdom
- G1001354/1/MRC_/Medical Research Council/United Kingdom
- SBF006\1078/WT_/Wellcome Trust/United Kingdom
- MR/P023444/1, MC_UU_12019/1/MRC_/Medical Research Council/United Kingdom
- PG/17/90/33415, SPG 2822621/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
