

Establishing 3D organoid models from patient-derived conditionally reprogrammed cells to bridge preclinical and clinical insights in pancreatic cancer
- PMID: 40462147
- PMCID: PMC12131615
- DOI: 10.1186/s12943-025-02374-y
Establishing 3D organoid models from patient-derived conditionally reprogrammed cells to bridge preclinical and clinical insights in pancreatic cancer
Abstract
Background: Pancreatic cancer is a highly lethal malignancy with limited treatment response. Despite advancements in treatment, systemic chemotherapy remains the primary therapeutic approach for over 80% of patients, with no established biomarkers to guide drug selection. Traditional two-dimensional (2D) culture models fail to replicate the tumor microenvironment, necessitating the development of more advanced models, such as three-dimensional (3D) organoid models.
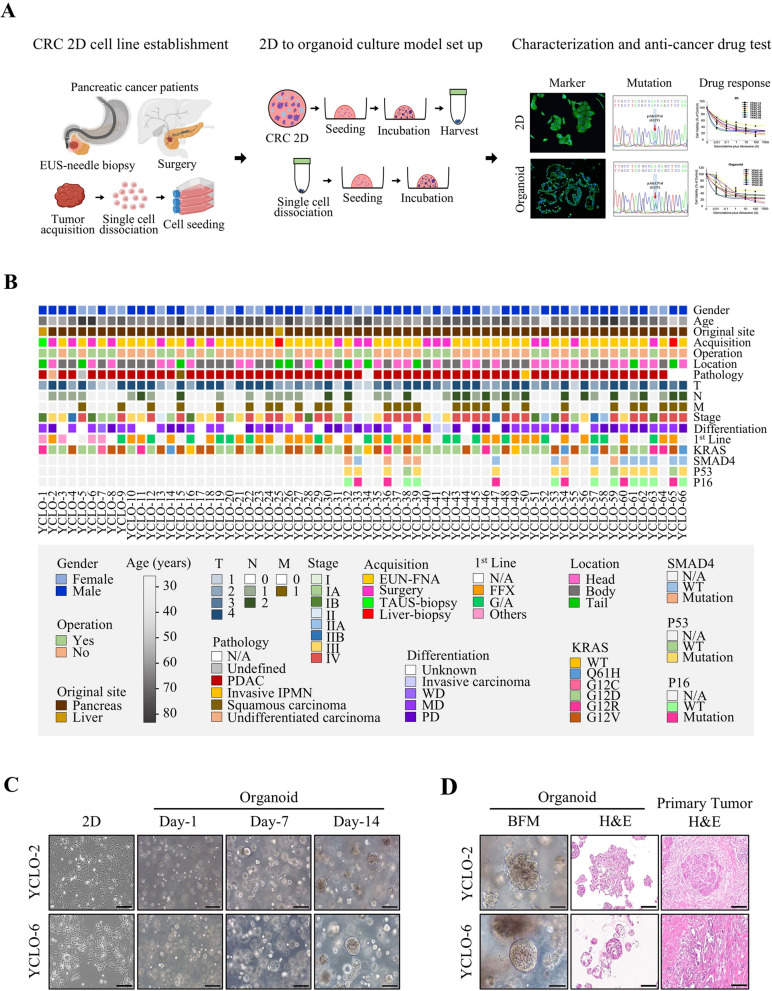
Methods: We established 3D organoid cultures using patient-derived conditionally reprogrammed cell (CRC) lines, originally cultured under 2D conditions. These CRC organoids were developed using a Matrigel-based platform without organoid-specific medium components to preserve the intrinsic molecular subtypes of the cells. Morphological, molecular, and drug sensitivity analyses were performed to compare the clinical responses of 3D CRC organoids with those of their 2D counterparts and clinical responses.
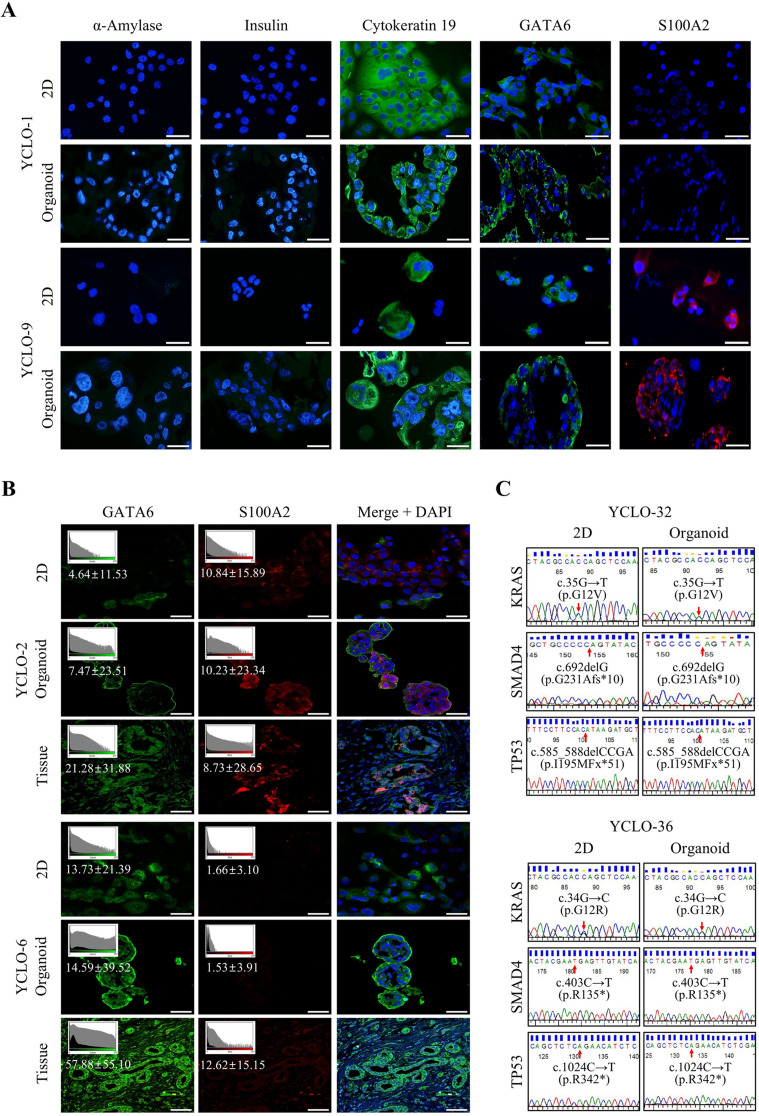
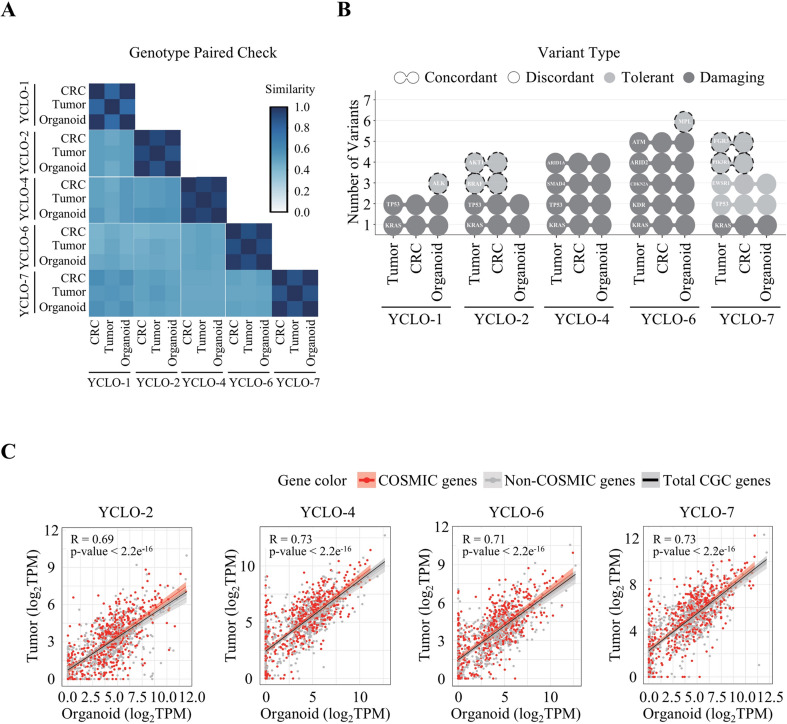
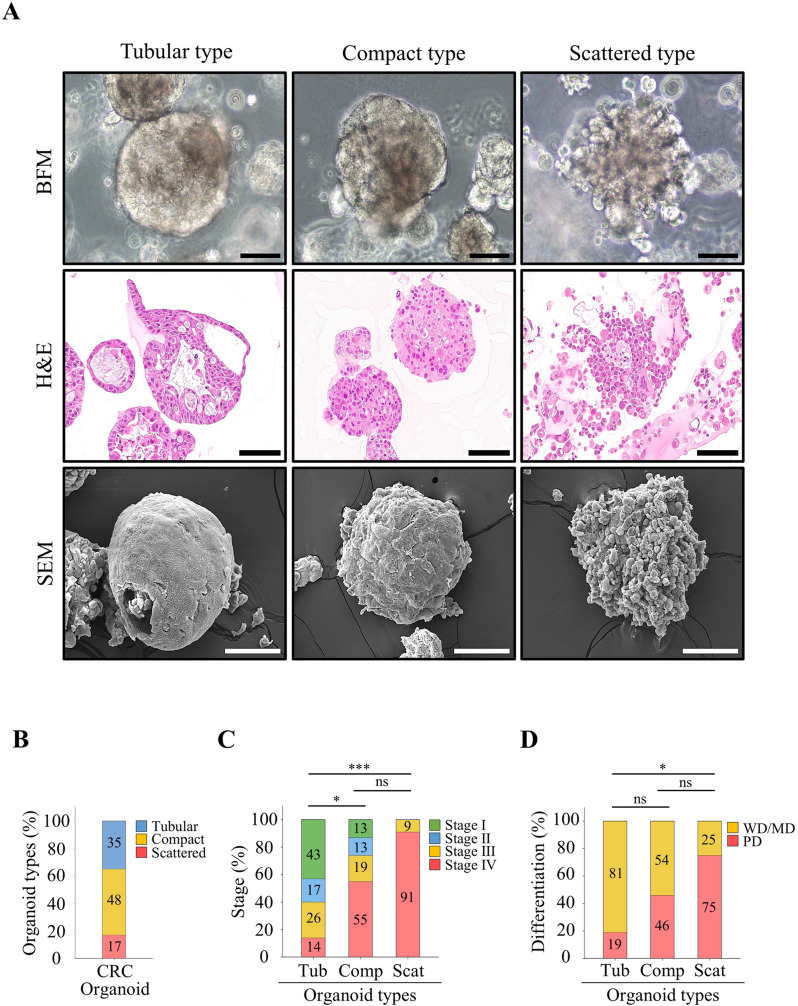
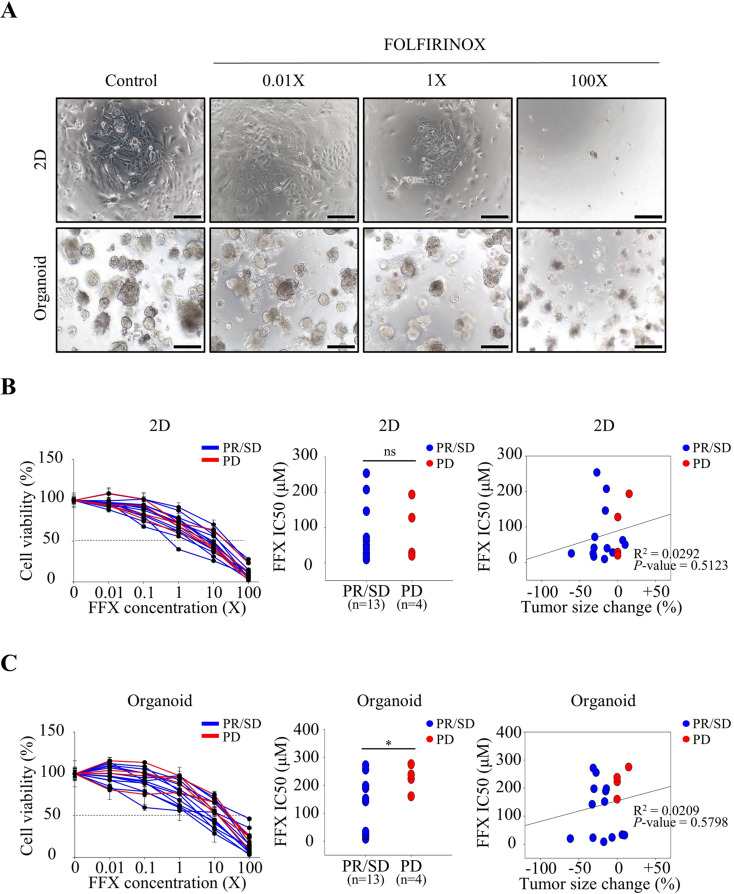
Results: The 3D CRC organoids retained the molecular characteristics, transcriptomic and mutational profiles of the parental tumors and displayed distinct morphologies corresponding to cancer stages and differentiation. Drug response profiling of gemcitabine plus nab-paclitaxel (Abraxane) and FOLFIRINOX demonstrated that the 3D organoids more accurately mirrored patient clinical responses than the 2D cultures. Notably, the IC50 values for the 3D organoids were generally higher, reflecting the structural complexity and drug penetration barriers observed in vivo.
Conclusion: Matrigel-based 3D organoid culture models provide a robust platform for pre-clinical drug evaluation, overcoming the limitations of 2D models. Although time- and resource-intensive, integrating both 2D and 3D platforms enables efficient initial screening and validation. This approach holds promise for identifying predictive biomarkers and advancing precision medicine in pancreatic cancer treatment.
Keywords: 3D organoid culture; Conditionally reprogrammed cell (CRC) organoids; Drug sensitivity screening; FOLFIRINOX; Gemcitabine plus nab-paclitaxel (Abraxane); Pancreatic cancer; Precision medicine.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Institutional Review Board of Yonsei University Medical Center (number 4-2019-0614). Consent for publication: Written informed consent was obtained from all the patients. Competing interests: The authors declare no competing interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
