

Delayed Laparoscopic Cholecystectomy With Fluorescent Cholangiography for Acute Cholecystitis: Is It Safe?
- PMID: 40462457
- PMCID: PMC12134524
- DOI: 10.1111/ases.70092
Delayed Laparoscopic Cholecystectomy With Fluorescent Cholangiography for Acute Cholecystitis: Is It Safe?
Abstract
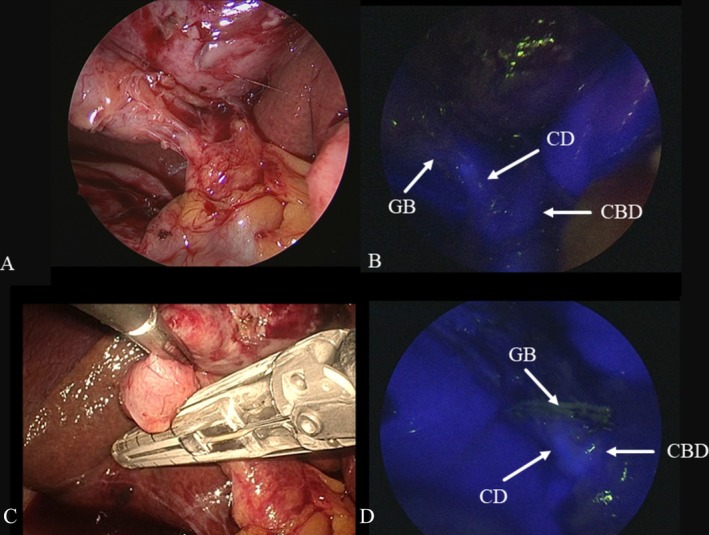
Background: According to the Tokyo Guidelines 2018 (TG-18), delayed laparoscopic cholecystectomy (DLC) after recovering from acute cholecystitis (AC) is recommended for patients with poor status. Moreover, DLC for patients with good status remains controversial, and TG-18 does not include clinical questions regarding fluorescent cholangiography (FC). In this study, we evaluated the clinical value and safety of FC during DLC.
Methods: We performed DLC in 226 patients after recovering from AC. The electronic medical records of these patients were retrospectively reviewed, focusing on preoperative assessment and intraoperative and postoperative outcomes. Biliary and/or arterial injuries were treated as intraoperative complications.
Results: Of the study patients, 144 underwent DLC with FC. Among the remaining 82 patients who underwent DLC without FC, the rate of intraoperative complications was 7.3% (n = 6), which was significantly higher than in those who underwent DLC with FC (0%) (p = 0.002). The rate of conversion to open cholecystectomy during DLC with FC (1.4%) was significantly lower than that during DLC without FC (15.9%). The mean operative time was not significantly different between the patients who underwent DLC with and without FC (p = 0.503). The mean blood loss and postoperative complications in patients who underwent DLC with FC were significantly lower than those who underwent DLC without FC (p = 0.041 and p = 0.002, respectively).
Conclusions: Utilizing FC can reduce intraoperative and postoperative complications, the conversion rate, and blood loss during DLC; therefore, DLC with FC is recognized as a safe procedure for patients with AC.
Keywords: acute cholecystitis; delayed laparoscopic cholecystectomy; fluorescent cholangiography; percutaneous transhepatic gallbladder drainage; single‐incision laparoscopic cholecystectomy.
Asian Journal of Endoscopic Surgery© 2025 The Author(s). Asian Journal of Endoscopic Surgery published by Asia Endosurgery Task Force and Japan Society of Endoscopic Surgery and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





Similar articles
-
Comparison of laparoscopic cholecystectomy and delayed laparoscopic cholecystectomy in aged acute calculous cholecystitis: a cohort study.Surg Endosc. 2020 Jul;34(7):2994-3001. doi: 10.1007/s00464-019-07091-4. Epub 2019 Aug 28. Surg Endosc. 2020. PMID: 31463722
-
Outcomes of early versus delayed laparoscopic cholecystectomy for acute cholecystitis performed at a single institution.Asian J Endosc Surg. 2019 Jan;12(1):74-80. doi: 10.1111/ases.12487. Epub 2018 Apr 3. Asian J Endosc Surg. 2019. PMID: 29611896
-
Risk factors for difficulty of laparoscopic cholecystectomy in grade II acute cholecystitis according to the Tokyo guidelines 2013.BMC Surg. 2017 Nov 28;17(1):114. doi: 10.1186/s12893-017-0319-6. BMC Surg. 2017. PMID: 29183352 Free PMC article.
-
Comparison of emergency cholecystectomy and delayed cholecystectomy after percutaneous transhepatic gallbladder drainage in patients with acute cholecystitis: a systematic review and meta-analysis.Updates Surg. 2021 Apr;73(2):481-494. doi: 10.1007/s13304-020-00894-4. Epub 2020 Oct 13. Updates Surg. 2021. PMID: 33048340 Free PMC article.
-
Laparoscopic cholecystectomy in acute cholecystitis: indication, technique, risk and outcome.Langenbecks Arch Surg. 2005 Sep;390(5):373-80. doi: 10.1007/s00423-004-0509-4. Epub 2004 Aug 14. Langenbecks Arch Surg. 2005. PMID: 15316783 Review.
References
-
- Okamoto K., Suzuki T., Takada T., et al., “Tokyo Guidelines 2018: Flowchart for the Management of Acute Cholecystitis,” Journal of Hepato‐Biliary‐Pancreatic Sciences 25 (2018): 55–72. - PubMed
-
- ASA Physical Status Classification System , “Last Approved by the ASA House of Delegates on October 15, 2014,” https://www.asahq.org/resources/clinical‐information/asa‐physical‐status....
-
- Abouleish A. E., Leib M. L., and Cohen N. H., “ASA Provides Examples to Each ASA Physical Status Class,” ASA Monitor 79 (2015): 38–39.
-
- Charlson M. E., Pompei P., Ales K. L., and MacKenzie C. R., “A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation,” Journal of Chronic Diseases 40 (1987): 373–383. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
