

Efficacy of neoadjuvant, adjuvant, and perioperative immunotherapy in non-small cell lung cancer across different PD-L1 expression levels: a systematic review and meta-analysis
- PMID: 40463367
- PMCID: PMC12129973
- DOI: 10.3389/fimmu.2025.1569864
Efficacy of neoadjuvant, adjuvant, and perioperative immunotherapy in non-small cell lung cancer across different PD-L1 expression levels: a systematic review and meta-analysis
Abstract
Background: Immune checkpoint inhibitors, particularly anti-PD-1/PD-L1 monoclonal antibodies, have transformed non-small cell lung cancer (NSCLC) treatment. This meta-analysis evaluates the efficacy of neoadjuvant, adjuvant, and perioperative immunotherapy in resectable NSCLC, stratified by PD-L1 expression levels.
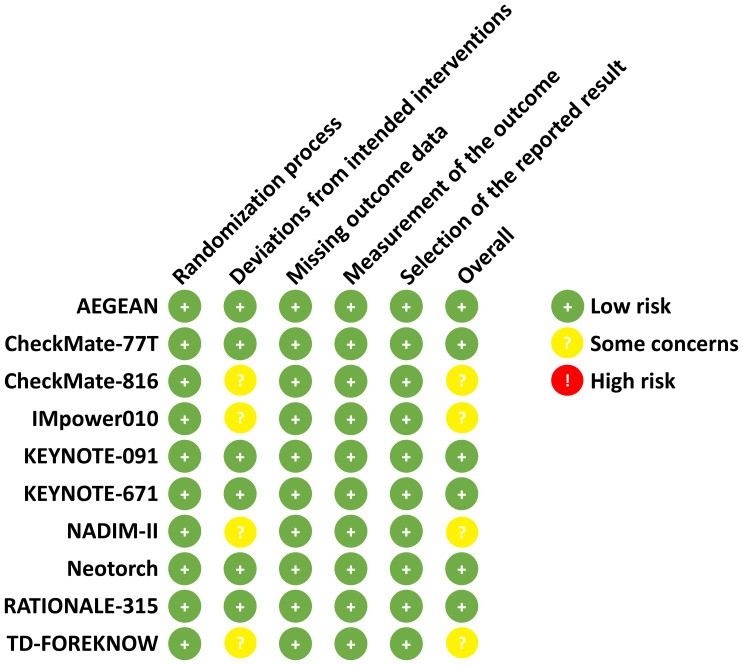
Methods: We conducted a meta-analysis of 10 randomized controlled trials (RCTs) involving 11 articles, focusing on pathological complete response (pCR), major pathological response (MPR), event-free survival (EFS), and overall survival (OS). These outcomes were stratified by PD-L1 expression levels (<1%, ≥1%, 1-49%, ≥50%).
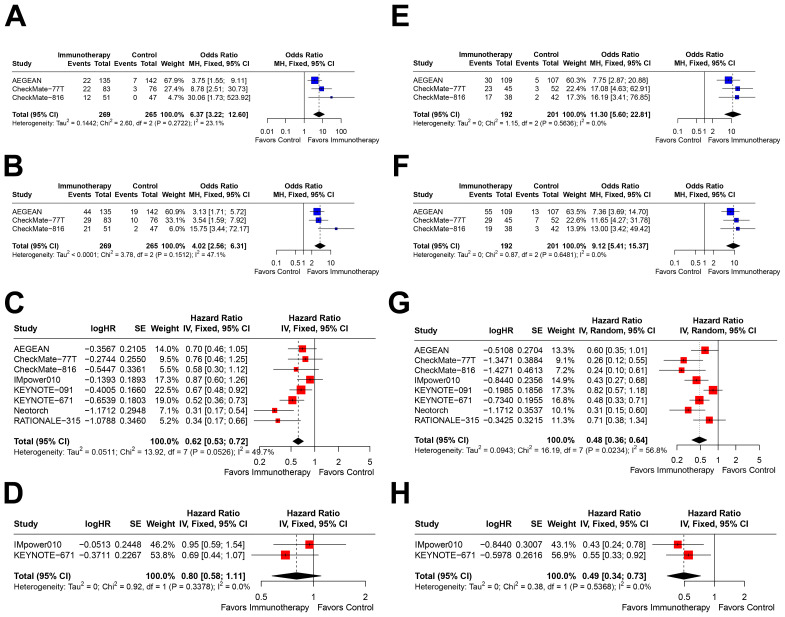
Results: Immunotherapy significantly improved pCR (OR=4.96, 95% CI=2.88-8.57 for PD-L1<1%; OR=9.58, 95% CI=6.32-14.53 for PD-L1≥1%), MPR (OR=2.86, 95% CI=1.97-4.16 for PD-L1<1%; OR=7.39, 95% CI=4.59-11.88 for PD-L1≥1%), and EFS (HR=0.80, 95% CI=0.70-0.92 for PD-L1<1%; HR=0.53, 95% CI=0.45-0.62 for PD-L1≥1%) across all PD-L1 subgroups. Greatest benefits were observed in PD-L1≥50% subgroup, with ORs for pCR and MPR, and HRs for EFS, showing consistent improvements. OS benefits were significant in PD-L1≥1% patients (HR=0.62, 95% CI=0.49-0.79 for PD-L1≥1%) but uncertain in PD-L1<1% cohorts (HR=1.11, 95% CI=0.86-1.44 for PD-L1<1%). Immunotherapy in perioperative setting demonstrated robust efficacy, with significant pathological response and EFS benefits across all PD-L1 subgroups.
Conclusion: This meta-analysis supports immunotherapy within perioperative care for resectable NSCLC, emphasizing PD-L1 expression as a predictive biomarker. Future studies should optimize patient selection and clarify immunotherapy's role in different treatment settings.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42025644497, identifier CRD42025644497.
Keywords: PD-L1 expression; efficacy; immunotherapy; meta-analysis; non-small cell lung cancer.
Copyright © 2025 Zhang, Lin and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials