

How to Do Echo for Noninvasive Hemodynamic Evaluation of the Patient in the Intensive Care Unit: A Consensus Statement of the Italian Society of Echocardiography and Cardiovascular Imaging
- PMID: 40463753
- PMCID: PMC12129274
- DOI: 10.4103/jcecho.jcecho_15_25
How to Do Echo for Noninvasive Hemodynamic Evaluation of the Patient in the Intensive Care Unit: A Consensus Statement of the Italian Society of Echocardiography and Cardiovascular Imaging
Abstract
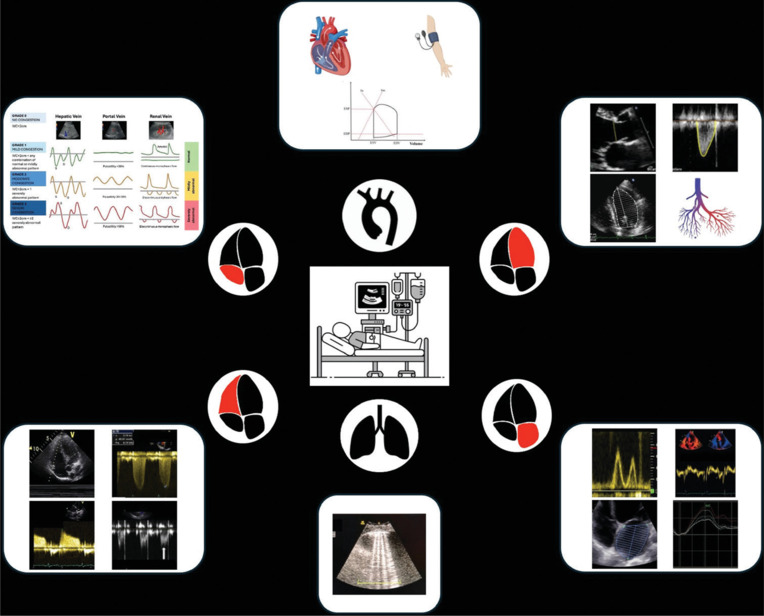
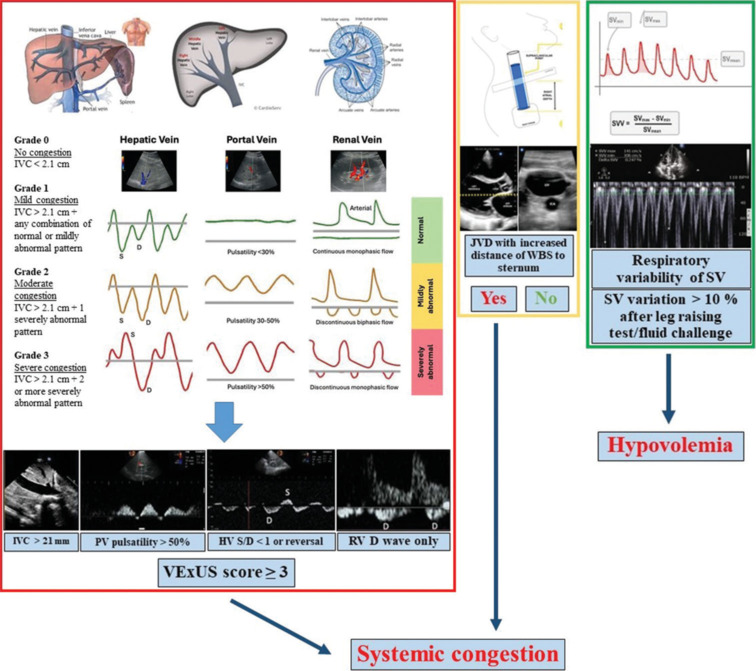
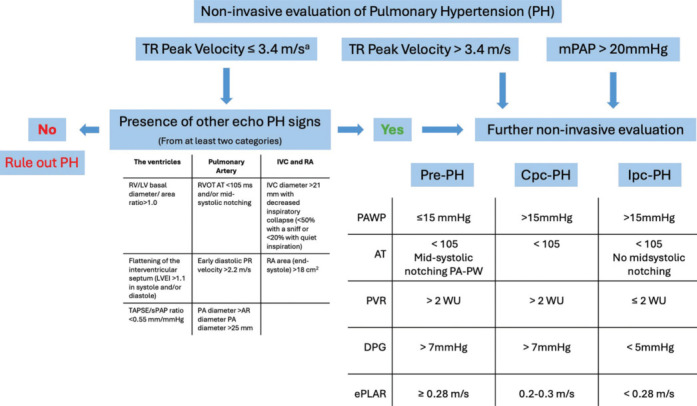
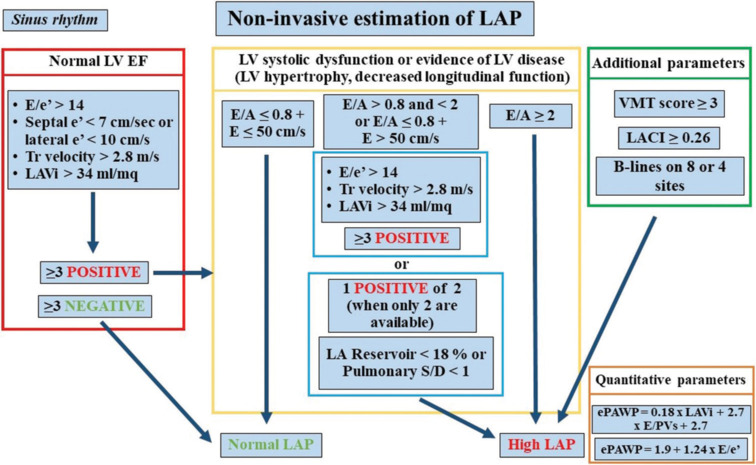
Critically ill patients in the intensive care unit (ICU) require continuous hemodynamic monitoring to guide therapeutic decisions and prevent clinical deterioration. Echocardiography has emerged as a cornerstone for noninvasive hemodynamic assessment, offering real-time, bedside evaluation of key parameters such as venous congestion, pulmonary pressures, left atrial pressure (LAP), systemic vascular resistances, cardiac output, and ventricular-arterial coupling. Systemic venous congestion and right atrial pressure (RAP) can be assessed through inferior vena cava diameter measurement and respiratory variation, with additional accuracy provided by the VeXUS score, which incorporates hepatic, portal, and renal vein Doppler profiles. Internal jugular vein assessment and left ventricular (LV) stroke volume variability further refine RAP estimation. Pulmonary hypertension (PH) and right ventricular dysfunction can be evaluated through echocardiographic markers that differentiate precapillary from postcapillary PH, enabling tailored treatment strategies. In addition, echocardiography is fundamental for detecting right ventricular failure, particularly in PH and cardiogenic shock. LAP and systemic hemodynamics are integral to assessing LV diastolic and systolic dysfunction, which are pivotal in heart failure and cardiogenic shock management. Echocardiography also provides insights into vascular system properties and their interaction with cardiac performance, while lung ultrasound aids in detecting interstitial edema of cardiac origin. As a fast, reliable, and reproducible tool, echocardiography is the gold standard for noninvasive hemodynamic assessment in ICU patients, facilitating prompt and precise therapeutic decisions.
Keywords: Echocardiography; hemodynamic monitoring; intensive care unit; left atrial pressure; noninvasive monitoring; pulmonary hypertension; right ventricular function; venous congestion.
Copyright: © 2025 Journal of Cardiovascular Echography.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685–713. - PubMed
-
- Soliman-Aboumarie H, Denault AY. How to assess systemic venous congestion with point of care ultrasound. Eur Heart J Cardiovasc Imaging. 2023;24:177–80. - PubMed
-
- Istrail L, Kiernan J, Stepanova M. A novel method for estimating right atrial pressure with point-of-care ultrasound. J Am Soc Echocardiogr. 2023;36:278–83. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials