

Stress Cardiomyopathy Complicated By Left Ventricular Thrombosis with Fatal Detachment
- PMID: 40463757
- PMCID: PMC12129268
- DOI: 10.4103/jcecho.jcecho_69_24
Stress Cardiomyopathy Complicated By Left Ventricular Thrombosis with Fatal Detachment
Abstract
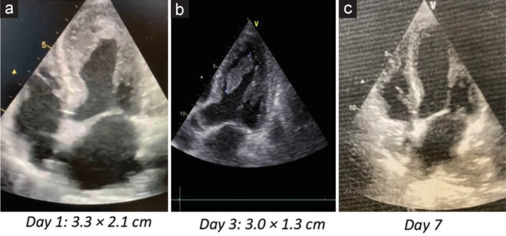
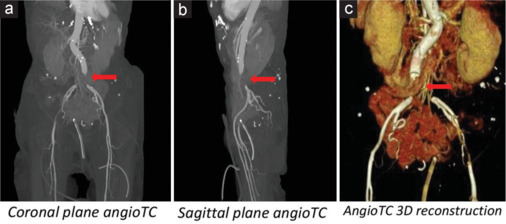
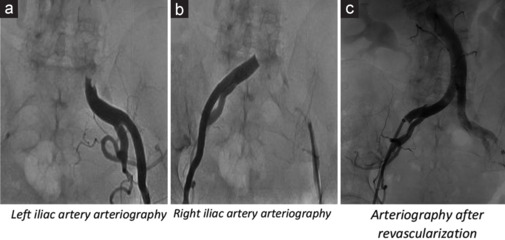
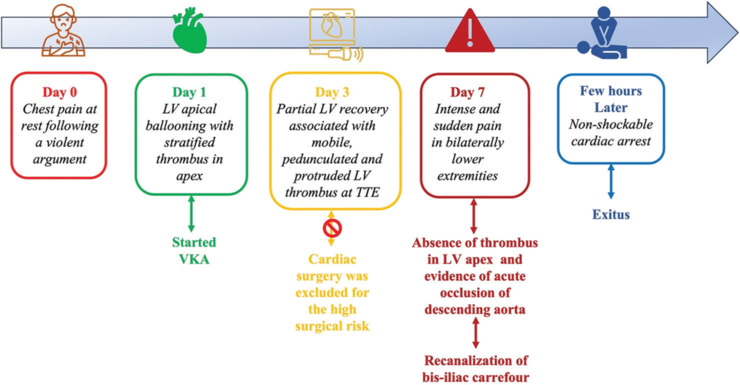
Left ventricular thrombosis (LVT) in stress cardiomyopathy or Takotsubo syndrome (TTS) is a moderately frequent complication. However, cardioembolic events are not frequently reported. Herein, we present a case report of 80-year-old patient admitted for chest pain at rest, started few days earlier following a violent argument. Her medical history included arterial hypertension and recent surgery of descending colon adenocarcinoma. Electrocardiogram showed sinus rhythm, negative T waves from V1 to V6, in D2, D3, AVF, and long QTc. Laboratory examinations documented an increased high sensitivity Troponin I, myoglobin, creatine kinase-MB, and B-type natriuretic peptide. Transthoracic echocardiography (TTE) showed a reduced left ventricular (LV) ejection fraction, "apical ballooning" with hyperkinesis of the basal segments of LV, suggestive for stress cardiomyopathy. A large thrombus in LV apex (3.3 cm × 2.1 cm) was found. Coronary angiogram showed normal coronary arteries. Anticoagulant therapy with Warfarin was quickly started, bridging with unfractionated heparin. Cardiac surgery was excluded for high-risk surgical patient. Daily TTE monitoring was done with evidence of slight reduction of the LVT. After 7th day from admission, the patient complained an intense and sudden pain in lower extremities bilaterally. An acute occlusion of the descending aorta just above the bifurcation in the common iliac arteries was found. Interventional radiology procedure of recanalization of the bis-iliac carrefour was successfully performed. However, few hours after the procedure, the patient's hemodynamic conditions worsened until the exitus.
Keywords: Acute thrombosis of descending aorta; anticoagulation; left ventricular thrombosis; stress cardiomyopathy; takotsubo syndrome.
Copyright: © 2025 Journal of Cardiovascular Echography.
Figures
References
-
- Lyon AR, Bossone E, Schneider B, Sechtem U, Citro R, Underwood SR, et al. Current state of knowledge on Takotsubo syndrome: A position statement from the taskforce on Takotsubo syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2016;18:8–27. - PubMed
-
- Levine GN, McEvoy JW, Fang JC, Ibeh C, McCarthy CP, Misra A, et al. Management of patients at risk for and with left ventricular thrombus: A scientific statement from the American Heart Association. Circulation. 2022;146:e205–23. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous