

Efficacy and safety of belimumab in lupus nephritis patients with nephrotic syndrome: a single-centre observational retrospective study
- PMID: 40463808
- PMCID: PMC12128045
- DOI: 10.1093/ckj/sfaf137
Efficacy and safety of belimumab in lupus nephritis patients with nephrotic syndrome: a single-centre observational retrospective study
Abstract
Background: Belimumab has been demonstrated to be efficient in improving the clinical outcome of patients with lupus nephritis (LN). However, evidence regarding its efficacy and safety in LN patients with nephrotic syndrome (NS) remains limited.
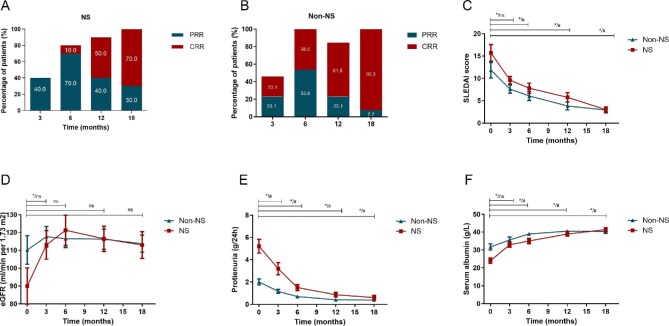
Methods: This retrospective study included 23 LN patients (10 with NS) treated with belimumab for 18 months. The renal response, including complete renal response (CRR), partial renal response (PRR) and the primary efficacy renal response (PERR), at month 18 and safety outcomes were assessed based on the 2024 Kidney Disease: Improving Global Outcomes LN guideline.
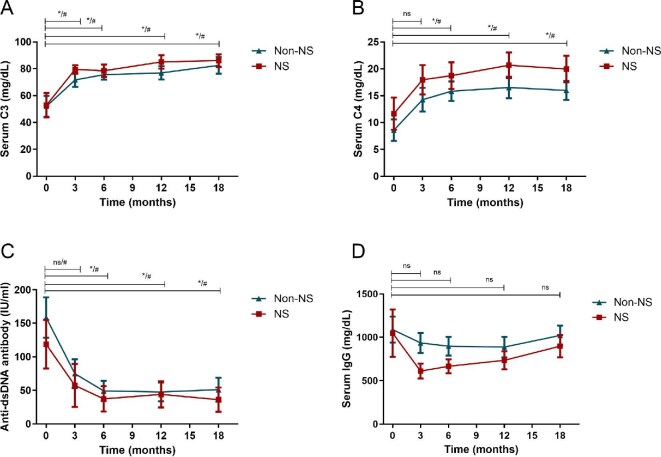
Results: Following the additional treatment with belimumab, all patients with NS achieved a renal response by month 18, with 30.0% PRR, 70.0% CRR and 80% PERR, which were comparable to those with non-NS (PRR: 30.0 versus 7.7%, P = .162; CRR: 70.0 versus 92.3%, P = .162; PERR: 80.0 versus 92.3%, P = .385). This improvement was accompanied by a significant reduction in proteinuria and Systemic Lupus Erythematosus Disease Activity Index score, as well as a significant improvement in levels of estimated glomerular filtration rate and serum C3/C4. Additionally, serum immunoglobulin G remained stable. Patients with NS successfully tapered the glucocorticoid (GC) dose from 36.0 mg (range 20.0-40.0) to 6.0 mg (range 4.0-8.5), with 50% of them reaching a GC dose of ≤6 mg/day at the last visit. Safety profiles were similar across both groups and no severe adverse events related to belimumab discontinuation or deaths were reported.
Conclusions: Belimumab showed comparable effectiveness and safety in LN patients with NS, providing valuable evidence for its real-world clinical use.
Keywords: belimumab; lupus nephritis; nephrotic syndrome; primary efficacy renal response; renal response.
© The Author(s) 2025. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
LinkOut - more resources
Full Text Sources
Miscellaneous
