

The use of telemedicine services for medical abortion
- PMID: 40464275
- PMCID: PMC12135146
- DOI: 10.1002/14651858.CD013764.pub2
The use of telemedicine services for medical abortion
Abstract
Rationale: Telemedicine models for medical abortion are service delivery models where care is provided by a health worker using telecommunications to support the abortion process. Existing evidence suggests that telemedicine for medical abortion is safe, effective, and acceptable to women compared to when care is provided in-clinic. However, the available data are often constrained by several factors. We sought to strengthen the evidence base by comparing telemedicine models for medical abortion with medical abortion provided in-clinic.
Objectives: To assess the safety, success rate, and acceptability of telemedicine models for medical abortion, according to which phase or phases (pre-abortion, abortion, and/or post-abortion) telecommunications were used as the primary means of service delivery, compared to in-clinic care for medical abortion in the corresponding phase/phases.
Search methods: We searched CENTRAL (Ovid EBM Reviews), MEDLINE ALL (Ovid), Embase.com, CINAHL (EBSCOhost), LILACS, Global Health (Ovid), Scopus, Google Scholar, and grey literature sources from the inception of the database to 13 August 2024. We screened the references of included studies and contacted authors to identify additional data or enquire about ongoing studies.
Eligibility criteria: We included randomised controlled trials (RCTs) and non-randomised studies (NRS) of telemedicine models compared with in-clinic care (standard care) for medical abortion. We only included studies that used an interactive type of telecommunication and studies where telemedicine services were provided by a health worker.
Outcomes: Critical: successful abortion (a terminated pregnancy without the need for surgical intervention to complete the abortion within 42 days of the abortion). Important: continuing pregnancy, blood transfusion, hospitalisation, emergency visits, satisfaction, adherence.
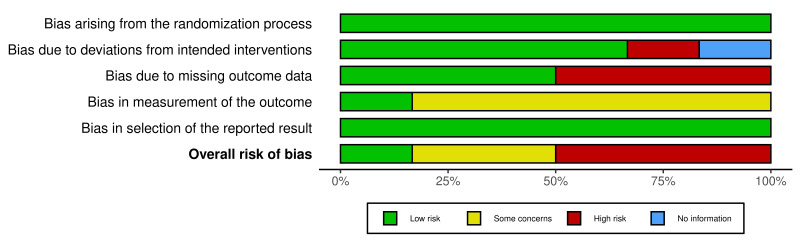
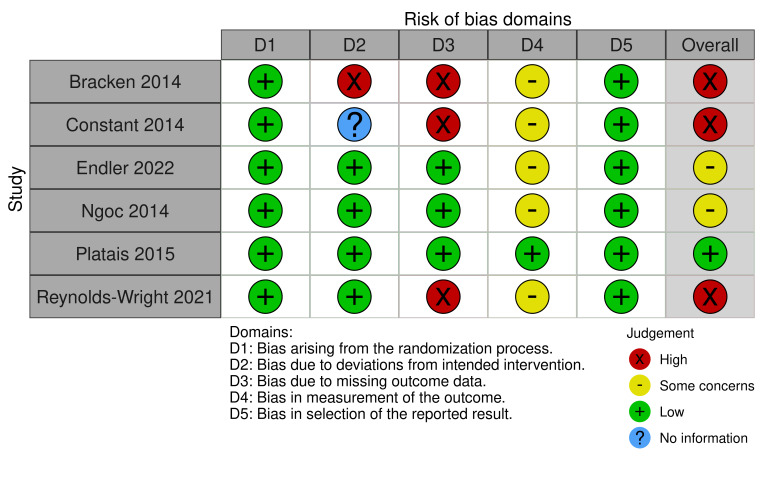
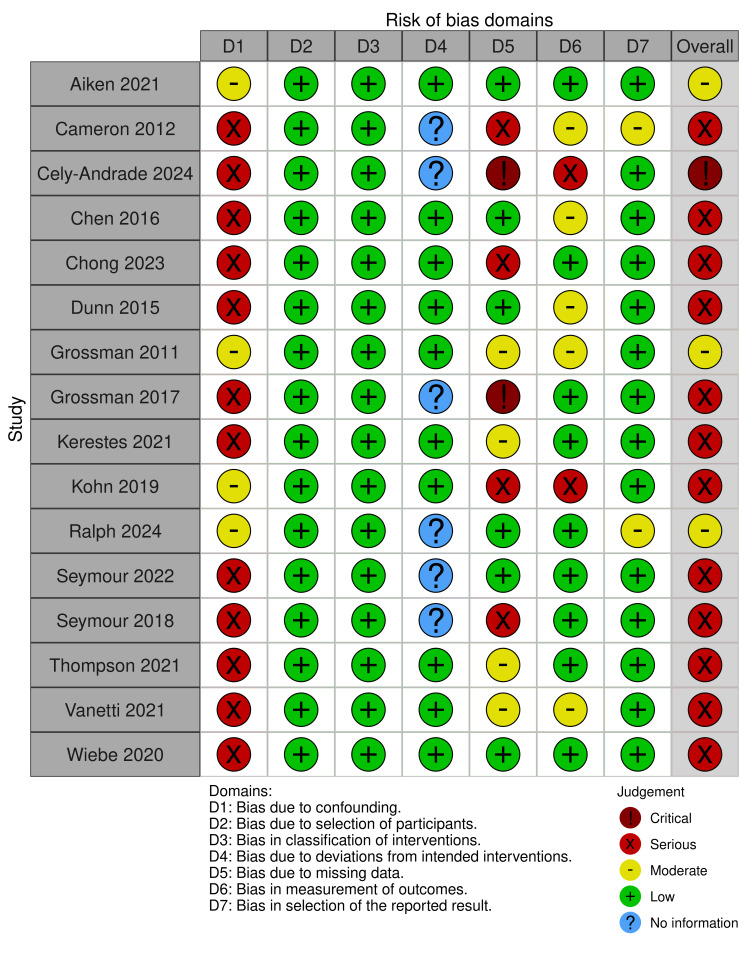
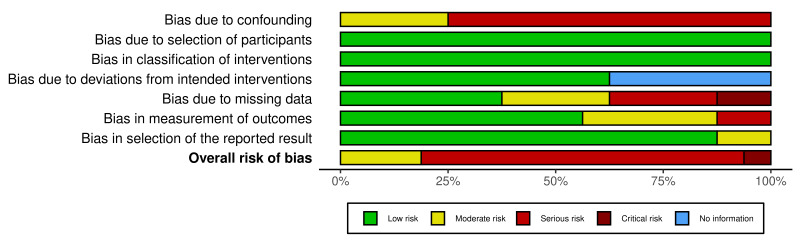
Risk of bias: We used the RoB 2 and ROBINS-I tools to assess the risk of bias in the included RCTs and NRS, respectively.
Synthesis methods: Two review authors (AC and ME) independently screened and extracted data in Covidence. We grouped interventions according to which abortion phase or phases (pre-abortion, abortion, post-abortion) telecommunications were used to deliver care. We graded the certainty of the evidence using the GRADE approach.
Included studies: We included 22 studies: six RCTs and 16 NRS, comprising a total of 131,278 individuals undergoing medical abortion up to 12 weeks' gestation. Studies were conducted across five high-income and four middle-income countries. Due to the heterogeneity among included NRS, we performed meta-analyses only for comparisons where we had RCTs.
Synthesis of results: Main intervention: Pre- to post-abortion care telemedicine models for medical abortion versus in-clinic care In these telemedicine models, various forms of synchronous and asynchronous telecommunications were used to deliver care from the pre- to post-abortion phase, up to 12 weeks' gestation. Any in-clinic testing was done to complement, rather than to replace, service delivery in the pre-abortion phase. Five out of nine studies did not perform routine ultrasounds as part of the eligibility screening. Pre- to post-abortion telemedicine models probably result in little to no difference in successful abortion (RR 0.99, 95% CI 0.97 to 1.01; 2 RCTs, 837 participants; moderate-certainty evidence). This finding was supported by NRS results (Aiken 2021; 99% versus 98%; adjusted P value = 0.268; 7 NRS, 83,061 participants; moderate-certainty evidence). Further, pre- to post-abortion telemedicine models probably result in little to no difference in rates of continued pregnancy (Aiken 2021: 0.5% versus 1%; adjusted P value = 0.268; 5 NRS, 74,269 participants; moderate-certainty evidence) and may result in little to no difference in blood transfusions (Aiken 2021: 0.02% versus 0.03%, adjusted P value = 0.557; 5 NRS, 83,651 participants; low-certainty evidence). The effect of the intervention on hospitalisation is uncertain (RR 1.45, 95% CI 0.24 to 8.61; 2 RCTs, 846 participants; very low-certainty evidence). This intervention may result in little to no difference in emergency visits (RR 1.15, 95% CI 0.36 to 3.75; 2 RCTs, 847 participants; low-certainty evidence) and satisfaction (RR 1.01, 95% CI 1.00 to 1.02; 2 RCTs, 832 participants; low-certainty evidence), and probably results in little to no difference in adherence to the medical abortion regimen (RR 0.99, 95% CI 0.96 to 1.02; 1 RCT, 732 participants; moderate-certainty evidence). No deaths were reported in this review. Sub-interventions: Pre-abortion/abortion telemedicine models for medical abortion versus in-clinic; Post-abortion telemedicine models versus in-clinic Four NRS compared pre-abortion/abortion telemedicine models with in-clinic care; all outcomes had very low-certainty evidence. Four RCTs and five NRS compared post-abortion telemedicine models with in-clinic follow-up. Post-abortion telemedicine models likely result in little to no difference in successful abortion (RR 1.0, 95% CI 0.99 to 1.01; 4 RCTs, 5069 participants; moderate-certainty evidence). They may result in little to no difference in continuing pregnancy (RR 0.81, 95% CI 0.48 to 1.36; 4 NRS, 5069 participants; low-certainty evidence) and likely result in higher rates of adherence to follow-up procedures (RR 1.15, 95% CI 1.13 to 1.18; 4 RCTs, 5235 participants; moderate-certainty evidence). The effects of post-abortion telemedicine models on blood transfusion, hospitalisation, emergency visits, and satisfaction are uncertain.
Authors' conclusions: Pre- to post-abortion telemedicine models probably result in little to no difference in successful abortion, continuing pregnancy, and adherence to the medical abortion regimen, with moderate-certainty evidence. We found low-certainty evidence that this intervention may result in little to no difference in rates of blood transfusions, emergency visits, and satisfaction, but we are uncertain about the effect on hospitalisation. Post-abortion telemedicine models likely result in higher rates of adherence to follow-up procedures, with moderate-certainty evidence. We downgraded studies mainly due to serious risk of bias or imprecision, with some outcomes being rare events. Altogether, the findings indicate that telemedicine models for medical abortion in early pregnancy may result in similar outcomes in terms of safety, effectiveness, and acceptability when compared to in-clinic provision. Most studies were conducted in high-resource settings and there were limited data on gestational ages above nine weeks. Future studies should investigate telemedicine models for medical abortion in lower-resourced settings and in gestational ages above nine weeks, compare different kinds of telecommunications, and assess models that omit testing (ultrasounds, physical exams, or blood tests).
Funding: None REGISTRATION: DOI: 10.1002/14651858.CD013764.
Copyright © 2025 The Authors. Cochrane Database of Systematic Reviews published by John Wiley & Sons, Ltd. on behalf of The Cochrane Collaboration.
Conflict of interest statement
AC: none known.
AL: none known.
KGD: has authored one of the included studies in this review (Endler 2022).
ME: has authored one of the included studies in this review (Endler 2022).
Figures

Update of
- doi: 10.1002/14651858.CD013764
Similar articles
-
Treatment for women with postpartum iron deficiency anaemia.Cochrane Database Syst Rev. 2024 Dec 13;12(12):CD010861. doi: 10.1002/14651858.CD010861.pub3. Cochrane Database Syst Rev. 2024. PMID: 39670550
-
Cell salvage for the management of postpartum haemorrhage.Cochrane Database Syst Rev. 2024 Dec 20;12(12):CD016120. doi: 10.1002/14651858.CD016120. Cochrane Database Syst Rev. 2024. PMID: 39704317
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Uterotonics for management of retained placenta.Cochrane Database Syst Rev. 2024 Oct 28;10(10):CD016147. doi: 10.1002/14651858.CD016147. Cochrane Database Syst Rev. 2024. PMID: 39465684
-
Surgical versus medical methods for second-trimester induced abortion.Cochrane Database Syst Rev. 2025 Jul 8;7(7):CD006714. doi: 10.1002/14651858.CD006714.pub3. Cochrane Database Syst Rev. 2025. PMID: 40626417 Review.
References
-
- Schmidt-Hansen M, Cameron S, Lohr PA, Hasler E. Follow-up strategies to confirm the success of medical abortion of pregnancies up to 10 weeks' gestation: a systematic review with meta-analyses. American Journal of Obstetrics and Gynecology 2020;222(6):551-63.e13. [DOI: 10.1016/j.ajog.2019.11.1244] - DOI - PubMed
-
- WHO. Abortion Care Guidelines. Geneva, Switzerland: World Health Organization, 2022.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials