

The Effect of an EHR Order Set on Cancer Screening Order Rates in Community-Based Health Centers
- PMID: 40467470
- PMCID: PMC12137202
- DOI: 10.1055/a-2524-5076
The Effect of an EHR Order Set on Cancer Screening Order Rates in Community-Based Health Centers
Abstract
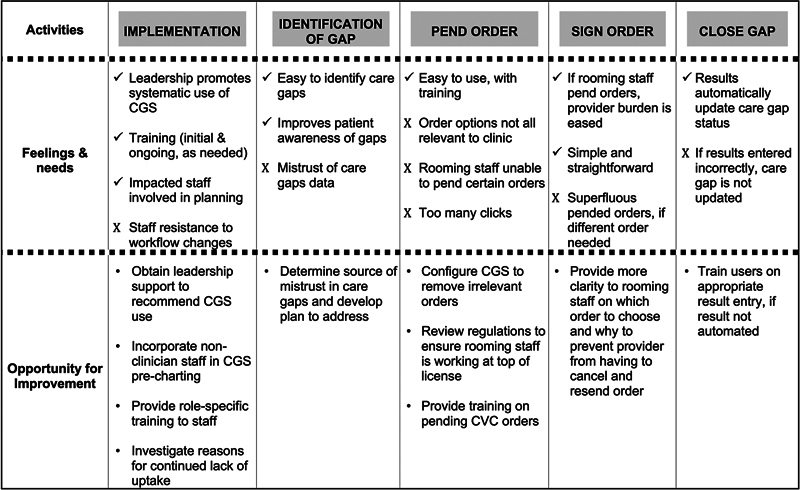
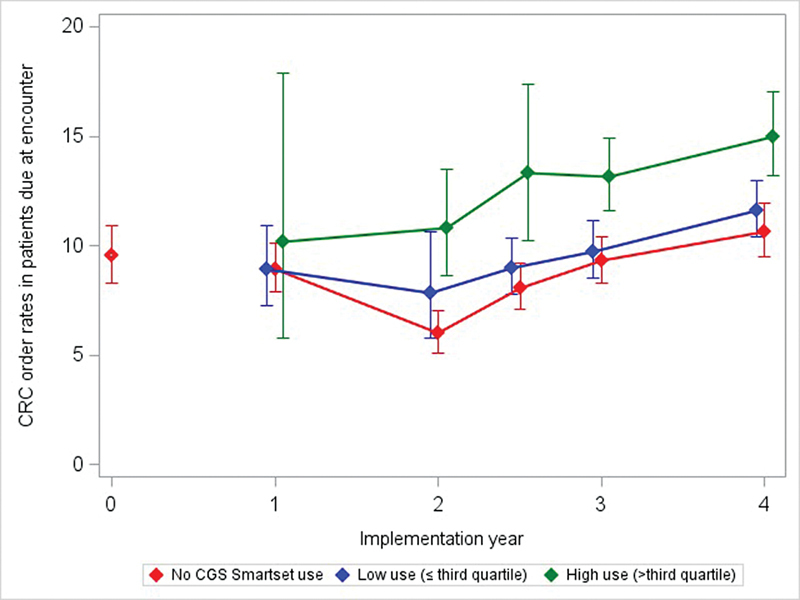
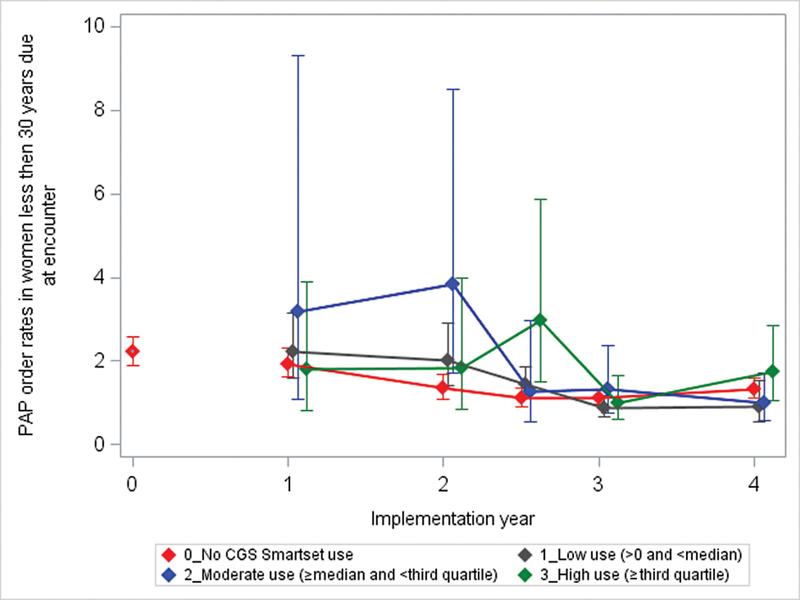
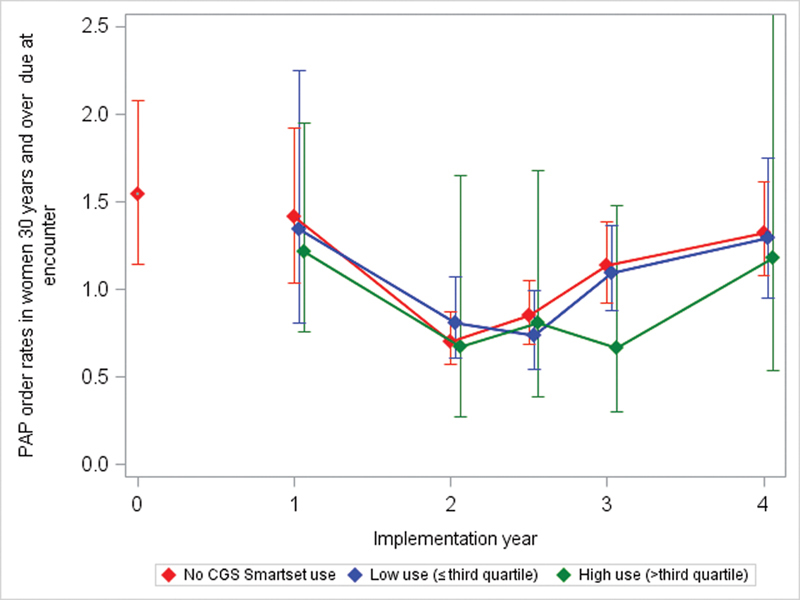
Adoption of electronic health record (EHR)-based clinical decision support tools in community-based health centers might increase the provision of indicated cancer screening orders. We examined: (1) if the use of the care gaps smartset (CGS), an EHR tool that expedites ordering care, is associated with colorectal/cervical cancer (CRC/CVC) screening order rates; and (2) how selected implementation strategies, barriers, and facilitators impact CGS use.Within a sequential mixed methods design, we used multivariate regression to assess associations between clinic- and provider-level CGS use and cancer screening order rates. Tool use rates (3/2018-12/2023) were measured as the rate of encounters at which any orders were placed via the CGS and then categorized by use level. Surveys (n = 81) and semi-structured interviews (n = 11) with clinic staff assessed strategies to improve tool use.Clinics and providers that ever used the CGS had higher CRC screening order rates than non-users. Higher CGS use was associated with better CRC screening order rates. By 12/2023, CRC screening orders were 4.4% (p < 0.05) higher in high-use clinics versus those with no CGS use. CGS use was not associated with CVC screening order rates. Qualitative findings indicate effective CGS use was enhanced by leadership support, clear workflows, and clinic-led training. Barriers to CGS use included low user awareness of/trust in the tool, and tool functions that were not optimized.CGS use can support cancer screening ordering; its adoption may be enhanced by varied training approaches and workflow design.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
None declared.
Figures
Similar articles
-
An observational study of workflows to support fecal testing for colorectal cancer screening in primary care practices serving Medicaid enrollees.BMC Cancer. 2022 Jan 25;22(1):106. doi: 10.1186/s12885-021-09106-7. BMC Cancer. 2022. PMID: 35078444 Free PMC article.
-
Colorectal Cancer Screening Rates at Community Health Centers that Use Electronic Health Records: A Cross Sectional Study.J Health Care Poor Underserved. 2015 May;26(2):377-90. doi: 10.1353/hpu.2015.0030. J Health Care Poor Underserved. 2015. PMID: 25913336
-
Effectiveness of a Mailed Colorectal Cancer Screening Outreach Program in Community Health Clinics: The STOP CRC Cluster Randomized Clinical Trial.JAMA Intern Med. 2018 Sep 1;178(9):1174-1181. doi: 10.1001/jamainternmed.2018.3629. JAMA Intern Med. 2018. PMID: 30083752 Free PMC article. Clinical Trial.
-
Development of a Field Guide for Assessing Readiness to Implement Evidence-Based Cancer Screening Interventions in Primary Care Clinics.Prev Chronic Dis. 2022 May 12;19:E25. doi: 10.5888/pcd19.210395. Prev Chronic Dis. 2022. PMID: 35550244 Free PMC article. Review.
-
Using implementation mapping for the adoption and implementation of Target:BP in community health centers.Front Public Health. 2022 Nov 24;10:928148. doi: 10.3389/fpubh.2022.928148. eCollection 2022. Front Public Health. 2022. PMID: 36504969 Free PMC article. Review.
References
-
- Healthy People 2030. Increase the proportion of adults who get screened for colorectal cancer—C-07. Accessed June 11, 2024 at:https://health.gov/healthypeople/objectives-and-data/browse-objectives/c...
-
- Healthy People 2030. Increase the proportion of females who get screened for cervical cancer—C-09. Accessed December 22, 2021 at:https://health.gov/healthypeople/objectives-and-data/browse-objectives/c...
-
- Gorina Y, Elgaddal N. Patterns of mammography, pap smear, and colorectal cancer screening services among women aged 45 and over. Natl Health Stat Rep. 2021;(157):1–18. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources