

Cancer prognosis and treatment results in patients with PTEN Hamartoma Tumour Syndrome (PHTS)-a European cohort study
- PMID: 40468016
- PMCID: PMC12137667
- DOI: 10.1038/s44276-025-00157-y
Cancer prognosis and treatment results in patients with PTEN Hamartoma Tumour Syndrome (PHTS)-a European cohort study
Abstract
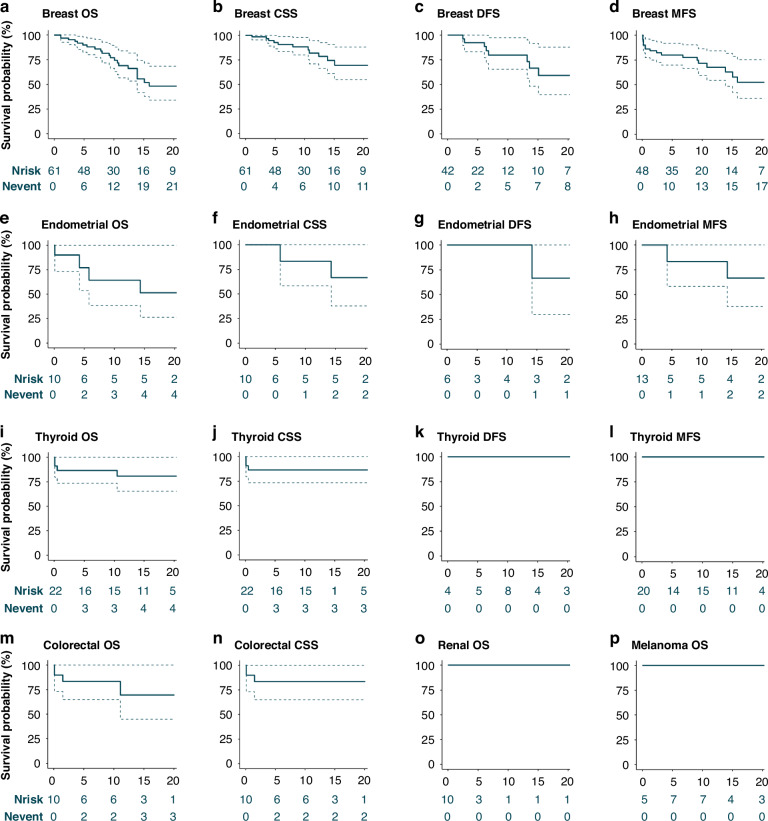
Background: PTEN hamartoma tumour syndrome (PHTS) patients have a high hereditary risk of cancer, especially breast (BC), endometrial (EC), and thyroid cancer (TC). However, the prognosis of PHTS-related cancers is unknown.
Methods: This European cohort study included adult PHTS patients with data from medical files, registries, and/or questionnaires. Overall survival (OS) was assessed using Kaplan-Meier analyses and were compared with sporadic cancer and the general population using standardized mortality (SMR) and relative survival rates (RSR). Survival bias was addressed using left-truncation.
Results: Overall, 147 BC patients were included. The 10y-OS was 77% (95%CI = 66-90), decreasing with increasing stage from 90% (95%CI = 73-100) for stage 0 to 0% (95%CI = 0-0) for stage IV. BC relative survival was comparable to sporadic BC in the first two years (2y-RSR = 1.1; 95%CI = 1.1-1.1) and increasing thereafter (5y-RSR = 1.7; 95%CI = 1.6-1.7). For TC (N = 56) and EC (N = 35), 10y-OS was 87% (95%CI = 74-100) and 64% (95%CI = 38-100), respectively. Overall and cancer-specific mortality in female PHTS patients exceeded general population rates (SMR = 3.7; 95%CI = 2.6-5.0 and SMR = 2.7; 95%CI = 1.6-4.4).
Conclusions: The prognosis of PHTS-related cancers was comparable to the general population. The higher overall mortality in PHTS patients is presumably related to their higher cancer incidence. These findings, and the high survival observed in early-stage cancer, emphasise the importance of recognising PHTS early to facilitate cancer surveillance.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.R.M. received funds from AstraZeneca for contribution to sponsored quality assessment and variant interpretation of VUS in BRCA1 and BRCA2. This funding was not related to this study. J.B. received funding support from GSK for an educational activity unrelated to this study. MT is the Editor-in-Chief of BJC Reports, he was not involved in any aspect of the handling of this manuscript or any editorial decisions. The remaining authors have no competing interests to declare. Ethics approval and consent to participate: This study was performed in accordance with the Declaration of Helsinki. The Research Ethics Committee of the Radboud university medical centre (file number 2018-5056) approved this study and the institutional ethics committees approved this study. Written informed consent was obtained when indicated by the ethics committee.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials